Information and resources for parents of trans-identified kids.
Part 1 – information
Firstly, this article isn’t going to tell you what I think you should do, because I don’t know what you should do. I don’t know you; I don’t know your child or your family situation. Appropriate decisions, approaches and solutions will be different for every family.
Not everyone reading this will have a child who believes that they have a brain/body mismatch, but most of you will know a child, or know of a child who identifies as trans or non-binary.
There are lots of articles out there telling us that these children should always be affirmed. They advise parents: tell your daughter she’s now your son; tell your son that yes, he’s a girl. You won’t have any trouble finding those pieces: organisations with hundreds of thousands of pounds of funding behind them perpetuate these ideas in schools and in the press, encouraging children to believe it is possible for a girl to grow up into a man, or for a boy to become a woman.
It can be hard to access information that questions this narrative. The affirmation model is new, and transition is not always a cure-all for the mental health issues that often accompany it.
Again, I am not trying to tell you what you should do.
I didn’t affirm my child. I told her I didn’t believe a boy could be born in a girl’s body and I didn’t believe that a girl could become a boy. I told her that idea was founded on regressive notions of sexism and stereotyping. This will not be the right approach for everyone and only you can decide how you’re going to proceed.
It might seem like an obvious thing to say but the most important thing is to keep channels of communication open and let your child know they are loved.
Let’s start with what I do know.
I do know how I felt when my 15 year old daughter handed me a piece of paper with “I’m transgender” written on it. In her mind at the time there was no doubt. She was certain that she was a boy somehow born into a girl’s body. What I felt wasn’t disgust, or anger, or disappointment, it was concern for my child and what the future might hold for her. It was overwhelming love, and sadness that she felt such confusion that she believed herself to be a boy and held such revulsion for her body that she believed she didn’t belong in it. Rejecting her was something that never crossed my mind.
I do know that most of the information I found online told me that it was essential to agree with her that she was a boy, use her ‘preferred pronouns’, find her a gender therapist and consider enabling access to puberty blockers, hormones and surgeries. To question this solution or consider other options was viewed as hateful: it was bigotry, it was transphobia. It was ‘conversion therapy’.
I do know that about nine months after she told me that she was actually a boy, my daughter desisted, and that in her own words:
I do know that my response to her feelings played only a part in her desistance and that it was a decision she came to on her own after a lot of soul searching.
You can read our story here. There is an increasing number of young people in the UK who are speaking out about desistence and detransition and I link to some of their voices later in this piece.
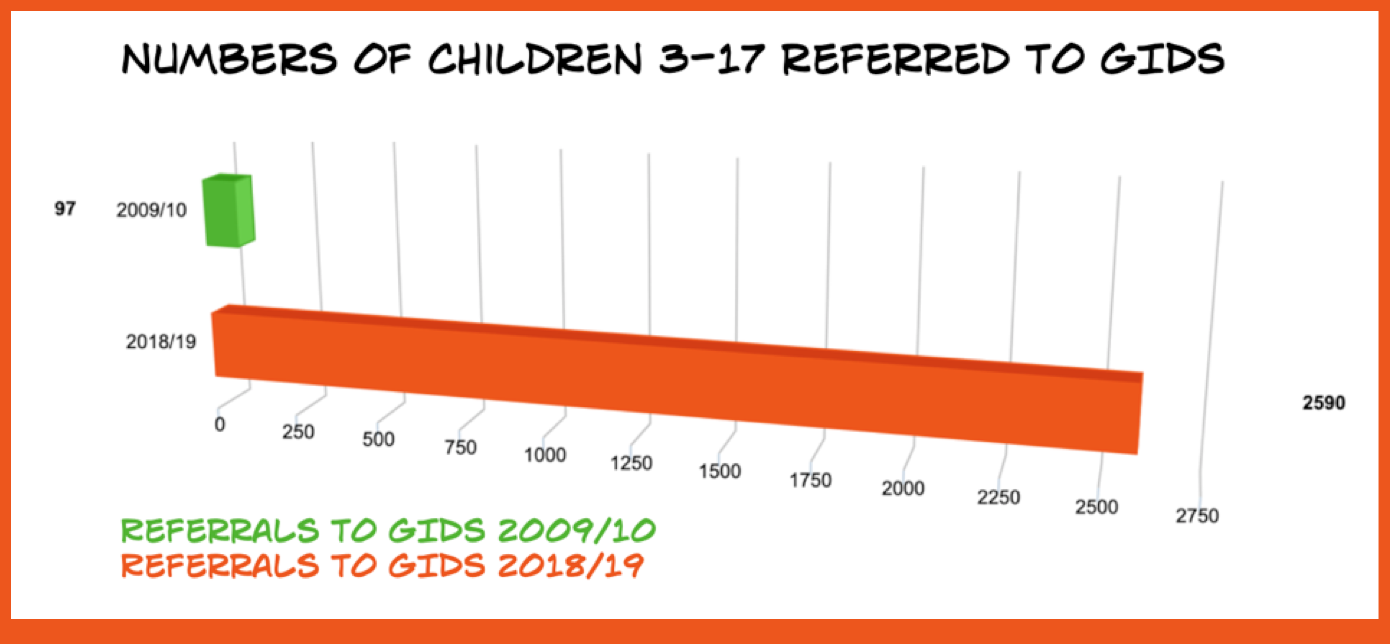
I do know that there has been an explosion in the numbers of children (aged 3-17) presenting to the GIDS (Gender Identity & Development Service) in the last decade. Referrals over the last nine years increased from 97 (2009/10) to 2590 (2018/19). Over 1,500 of these most recent referrals were aged 14-16.
 There are important questions to be asked and discussions to be had, concerning both child autonomy and child safeguarding, and the current political climate does not support this debate.
There are important questions to be asked and discussions to be had, concerning both child autonomy and child safeguarding, and the current political climate does not support this debate.
This is an article in two parts. Part one is an introduction, dealing with some of the key topics surrounding trans-identified young people. The trans-train has many carriages, so bear with me while we take a little trip through them.
The second part of the article, which will be published separately, contains resources, websites, podcasts and videos that deal with the potential problems with transition and the issues that are so often swept under the table in the rush to affirm a child’s gender identity.
PART ONE
The increase in trans-identified young people
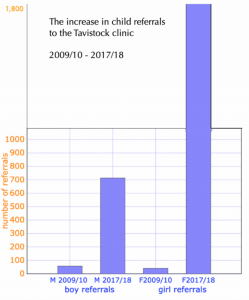 More young people than ever are identifying as transgender. This graph, which covers the last ten years, is based on the Tavistock GIDS own figures. You can check them yourself. Here is the data from 2009/10 to 2015/16 and here is the data from 2017/18.
More young people than ever are identifying as transgender. This graph, which covers the last ten years, is based on the Tavistock GIDS own figures. You can check them yourself. Here is the data from 2009/10 to 2015/16 and here is the data from 2017/18.
You may be surprised that more concern is not being raised about these figures. So am I.
Some people claim that prior to recently, young people did not ‘have the words’ to explain that they were trans, and that explains the increase.
Many children who identify as trans have previously come out as lesbian or gay. Many have social media addictions, some are high achievers or on the autistic spectrum. Some self-harm, some have been sexually abused. Some suffer from depression or other mental health issues. All or none of these factors may be present. Some therapists see transition as a ‘cure all’ for many of these other issues. Others are concerned that gay or lesbian children are being offered transition as a ‘cure’ for their own internalised homophobia, or for other problems, and that transition is merely putting a plaster over a wound.
Many believe social contagion plays a huge part in the increase, via the pressures of social media and the increased online sexualisation of girls. Groups such as Mermaids now go into schools and tell kids as young as five that we all have an innate ‘gender identity’. Children are told that they can choose whether to be a girl or a boy. Some groups claim that if you don’t have a gender identity it’s because you’re happy with the one you were ‘assigned at birth’, which is indeed a Catch 22 situation. I write about this extensively elsewhere on my blog, in ‘but nobody is encouraging kids to be trans!’.
ROGD
Traditionally, the very small number of trans-identified children were almost entirely boys, who suffered gender dysphoria from early childhood. That pattern has changed and, as you can see on the graph above, girls now make up the vast majority of referrals.
Rapid Onset Gender Dysphoria (ROGD) occurs when a child who has shown no prior signs of believing themselves to be ‘born in the wrong body’ suddenly identifies as transgender at or around puberty.
 Despite many young people, and even more parents, having reported experience of ROGD, most groups established to help transgender young people staunchly refuse to acknowledge its existence, insisting that if a child says they are trans then they are trans, and that a refusal to accept this is harmful and abusive.
Despite many young people, and even more parents, having reported experience of ROGD, most groups established to help transgender young people staunchly refuse to acknowledge its existence, insisting that if a child says they are trans then they are trans, and that a refusal to accept this is harmful and abusive.
This does not explain the existence of detransitioners, nor the desistence rates of up to 80% that have been traditionally noted in children attending GIDS and other clinics.
To dismiss parents who observe ROGD in their own children by claiming they simply hadn’t noticed prior signs that their child was trans- that the child had kept it secret from them or even that the child themselves hadn’t realised- is simplistic and unlikely. This argument is grounded in the idea of bad or inadequate parenting and assumes a closed and unproductive relationship with the child.
 Academic Lisa Littman, Assistant Professor of the Practice at the Brown University School of Public Health, carried out a study on ROGD in 2018. You can read an interview with Littman, where she discusses her work and the response to it, here.
Academic Lisa Littman, Assistant Professor of the Practice at the Brown University School of Public Health, carried out a study on ROGD in 2018. You can read an interview with Littman, where she discusses her work and the response to it, here.
You can read my own ROGD article here.
Social media and the internet
Where to begin with the omniscient power of social media? Those of us over thirty may have trouble understanding the extent to which it monopolises the lives of many young people who have never known a world without it. Some of us may understand it better than we would like to admit.
Online you can be whoever you choose to be: a better, shinier, idealised you. Online you can easily create the identity of your choice and most kids spend so much time online that it is hardly surprising the boundaries between real life and virtual life become blurred.
This is a state of hyperreality, which definitions.net describes as “an inability of consciousness to distinguish reality from a simulation of reality, especially in technologically advanced post-modern societies.”
There are plenty of young people their own age ready to cheer them on, on Instagram and other platforms.
You don’t even have to feel you should have been born the opposite sex: you can join the gender fluid, who sometimes feel like boys and sometimes like girls, or the non binary who feel neither like boys or girls…
How are these kids computing what a boy or a girl is supposed to feel like? Which boy or girl? On what day? What stereotypes are these decisions being based upon?
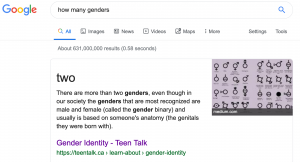 When I typed ‘how many genders’ into Google, the top hit of the six hundred and thirty one million that it threw up in less than a second told me this:
When I typed ‘how many genders’ into Google, the top hit of the six hundred and thirty one million that it threw up in less than a second told me this:
“There are more than two genders… gender isn’t about someone’s anatomy, it is about who they know them self to be. There are many different gender identities, including male, female, transgender, gender neutral, non-binary, agender, pangender, genderqueer, two-spirit, third gender, and all, none or a combination of these.”
So there we have it. Oh, wait, there’s more.
“There are many more gender identities then we’ve listed. Gender can be complex…”
It seems it can, and it certainly isn’t just youngsters worshiping at the temple of the gender fairy.
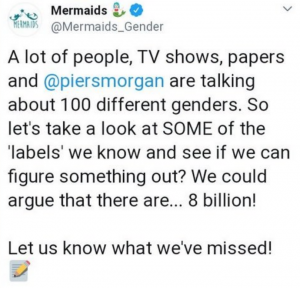
Mermaids speculated on Twitter earlier this year that there might be eight billion genders. Just imagine! More genders than people on the planet!
Earlier this year it was also confirmed that Mermaids had been awarded a £500,000 ‘Reaching Communities’ grant from the National Lottery.
“Mermaids provides trans-inclusive diversity training to schools, organisations, health professionals, public bodies and private companies.” proclaims the Mermaids website.
 Even the government’s own Office for National Statistics (ONS) is playing the gender game. It has this to say on the subject:
Even the government’s own Office for National Statistics (ONS) is playing the gender game. It has this to say on the subject:
“Growing numbers of people are identifying as somewhere along a continuum between man and woman, or as non-gendered (neither man nor woman) … an individual may see themselves as a man, a woman, as having no gender, or as having a non-binary gender – where people identify as somewhere on a spectrum between man and woman“.
Confused? Don’t worry.
YouTube
YouTube is full of ‘my transition timeline’ videos with thousands of hits, where trans-identified youngsters celebrate the glory of their new lives. “My FtM Top Surgery Consultation At 14!” for example, has over 52,000 views and comments such as, ‘You look so masculine and your voice is so deep. I’m so proud of how far you’ve come‘ and others bemoaning how their ‘unsupportive parents’ won’t cough up the necessary cash. ‘Tips on how to dress to pass better FTM’ has 86,000 views and comments include ‘don’t wear red flannel, u will be mistaken for a lesbian’ and ‘your voice is so deep! I’m jealous’. But that’s just the tip of the iceberg. Ash Hardel’s video ‘Calling my mom to tell her I’m trans‘ has – wait for it – over twelve million views.
You can read more about the power of social media influencers in my post ‘but nobody’s encouraging kids to be trans!’.

If you think your child is spending too much time online, encourage them to switch off and spend more time in touch with the physical world. I know that can be easier said than done. Can you go on a long walk with your child, or even an outdoor holiday? Can they leave their phone plugged in in the hall at bedtime? Can you turn off the wifi at night? Ask your child to think over the course of a few days about how going online really makes them feel. Some studies suggest that most of us feel more anxious after spending time on social media.
A September 2019 study of over 6,000 American teenagers showed that those who spent more than three hours a day on social media were ‘more likely to develop mental health problems including depression, anxiety, aggression, and antisocial behavior’.
Suicide
 Child suicides are thankfully incredibly rare. The idea that trans-identified children will kill themselves if not transitioned is irresponsibly promoted on television, on websites, in interviews and perpetuated by the media and transgender ‘support’ groups. It is almost as if the idea of suicide ideation is marketed to confused and unhappy children as a bargaining and silencing tool and an essential facet of a trans-identity. Such reporting contravenes Samaritans guidelines, whose research shows links between media coverage of suicide and increases in suicidal behaviour.
Child suicides are thankfully incredibly rare. The idea that trans-identified children will kill themselves if not transitioned is irresponsibly promoted on television, on websites, in interviews and perpetuated by the media and transgender ‘support’ groups. It is almost as if the idea of suicide ideation is marketed to confused and unhappy children as a bargaining and silencing tool and an essential facet of a trans-identity. Such reporting contravenes Samaritans guidelines, whose research shows links between media coverage of suicide and increases in suicidal behaviour.
You can read Transgender Trend’s piece ‘Suicide Facts and Myths‘ here.
If a young person is threatening suicide there are likely to be multiple reasons. If you feel your child may be suicidal, seek help as soon as possible from a professional who is willing to look at the bigger picture. Help for suicidal thoughts should be sought from counsellors trained specifically in this area.
Social transition
 There have been nearly a dozen studies undertaken into gender dysphoria and desistance. Current evidence suggests that following the traditional path of ‘watchful waiting’ around 80% of children outgrow gender dysphoria by the end of puberty, and that many grow up to be lesbian or gay. The new fashion is for ‘affirmation’, changing pronouns and perpetuating the idea that a girl is actually a boy or vice versa.
There have been nearly a dozen studies undertaken into gender dysphoria and desistance. Current evidence suggests that following the traditional path of ‘watchful waiting’ around 80% of children outgrow gender dysphoria by the end of puberty, and that many grow up to be lesbian or gay. The new fashion is for ‘affirmation’, changing pronouns and perpetuating the idea that a girl is actually a boy or vice versa.
Is social transition more likely to lead to a child following the route of puberty blockers, which almost inevitably lead to cross sex hormones and potential sterility?
 “For some families the social transition can work as a kind of ‘it’s all going to be fine’ and actually the system is way more complicated than that.”
“For some families the social transition can work as a kind of ‘it’s all going to be fine’ and actually the system is way more complicated than that.”
Dr Bernadette Wren, Gender Identity Development Service (GIDS) at the Tavistock
“We have never recommended complete social transitioning” said Polly Carmichael of GIDS, “but it has become a really popular thing and many advocacy groups really promote it.”
Earlier this year, five clinicians resigned from the Tavistock, asserting that charities such as Mermaids were having a harmful effect by allegedly promoting transition as a cure-all solution for confused adolescents.
We are told that children as young as six are attending school ‘incognito’ as the opposite sex. This is especially concerning in the light of one study which suggests that children up to the age of seven may believe that a boy who puts on a dress literally becomes a girl. Can children this young really understand the concept of ‘gender identity’?
“It is beyond children’s cognitive abilities to understand the biological impossibility of a male child growing up to become an adult woman or a female child growing up to become an adult man, that a ‘girl’ is not who you are, but what you are and that no amount of medical innovation can change the biological reality.” writes Davies-Arai.
 “Unquestioning affirmation of a child’s belief is not a neutral act of kindness, but an active intervention that shapes and changes a child’s understanding and development. Affirmation by trusted adults forms or reinforces a child’s perception of reality. Living, and being affirmed daily as the opposite sex will affect and change the child’s developing sense of self, which risks creating a self-fulfilling prophesy.”
“Unquestioning affirmation of a child’s belief is not a neutral act of kindness, but an active intervention that shapes and changes a child’s understanding and development. Affirmation by trusted adults forms or reinforces a child’s perception of reality. Living, and being affirmed daily as the opposite sex will affect and change the child’s developing sense of self, which risks creating a self-fulfilling prophesy.”
Some GIDS psychologists assert that parents risk psychologically damaging their children by allowing them to socially transition. Others fear schools are rushing to allow pupils to change their names, uniforms and gender pronouns as soon as they “got a whisper that a child might be querying their identity”.
“Where are the parents in all of this?” asks Madeline Kearns in the Spectator. “They are often not told if their child is worried about their gender. During my (teacher) training, we were told to avoid ‘outing’ potential transgender children to their families. If the child so wished, we might want to keep mummy and daddy out of the loop.”
“There is no way that professionals can possibly pass on concerns… without being considered transphobic or bigoted,” a Child Protection officer told Jo Bartosh. “Many of us share the same concerns… I see children changing their name, turning against their family, rewriting their past.”
While GIDS clinicians concur that children should be allowed to explore behaviours more usually associated with the opposite sex (such as clothing or types of play) many agree that actions such as changing a child’s pronouns and affirming a child in the idea that they can ‘change gender’ can be harmful. They warn that ‘to formally socially transition before puberty risks pre-determining the outcome’.
 If you aren’t letting your child cut/grow their hair and dress (within reason) in clothes they choose themselves, ask yourself why not? If you’re forcing your daughter to do ballet, or your son to play football, encouraging a girl with no interest in performing femininity to “make herself pretty” or berating a sensitive boy to “man up”, this may be part of the problem. Gender roles are everywhere and often we don’t even consciously notice them. While many people slip fairly happily into the behaviours and clothing choices society expects from them, many don’t. And that’s just fine. There are plenty of happy, successful and super-cool people who don’t ‘perform masculinity or femininity’. Sometimes, but not always, they’re gay.
If you aren’t letting your child cut/grow their hair and dress (within reason) in clothes they choose themselves, ask yourself why not? If you’re forcing your daughter to do ballet, or your son to play football, encouraging a girl with no interest in performing femininity to “make herself pretty” or berating a sensitive boy to “man up”, this may be part of the problem. Gender roles are everywhere and often we don’t even consciously notice them. While many people slip fairly happily into the behaviours and clothing choices society expects from them, many don’t. And that’s just fine. There are plenty of happy, successful and super-cool people who don’t ‘perform masculinity or femininity’. Sometimes, but not always, they’re gay.
“Trans the gay away”
 While some trans advocacy groups accuse parents who don’t affirm their child’s transition of conversion therapy, many of us see the opposite as true. People who feel their gods may have a problem with homosexuality, or who feel uncomfortable with it themselves, may feel more comfortable with a ‘born in the wrong body’ narrative. Converting your gay child into a straight trans child may seem a viable option, especially if the idea is instigated by the child itself.
While some trans advocacy groups accuse parents who don’t affirm their child’s transition of conversion therapy, many of us see the opposite as true. People who feel their gods may have a problem with homosexuality, or who feel uncomfortable with it themselves, may feel more comfortable with a ‘born in the wrong body’ narrative. Converting your gay child into a straight trans child may seem a viable option, especially if the idea is instigated by the child itself.
Many trans people report that their parents and peers were unhappy with their inability to perform the gender stereotypes required of their sex. Sometimes they had homophobic parents or they themselves hated the idea of being gay. Paris Lees (MTF) says he was bullied at school for being ‘too weak to fight back’ and that his dad mocked his accent and accused him of “talking like a poof“. Munroe Bergdorf (MTF) called one of his Twitter followers a “hairy barren lesbian” and expressed a desire to ‘gay bash’ a TV star. Alex Bertie (FTM) told Janice Turner of the Times. “I was known as the ‘weird lesbian girl’ and nobody would speak to me… my sexuality tainted their perception of me entirely”. After declaring herself a boy she found, “suddenly, my teachers looked out for me in class.”
In an article in the METRO this month, transactivist Owl writes,“I was six years old when I was first told I was a sissy, because I threw a basketball ‘like a girl,” causing academic Susan Matthews to observe that the idea of ‘throwing like a girl’ is a misogynist comment that also hurts girls. Embracing the stereotypes, such as ‘girls throw basketballs badly’ seems to be at the heart of an ideology which goes nowhere without emphasis on clothing, hair and make up choices; which hobbies someone enjoys and how bad or good they are at certain things.
One of the clinicians who recently resigned from the Tavistock recently told the Times “many children decided they wanted to change gender after suffering homophobic bullying”.
Strong Lesbian Role Models
 Our culture is still incredibly homophobic and hetronormative. When mainstream TV series do celebrate lesbians they can be amazing- but they are always pretty, skinny and pert: think Willow and Tara, Waverley and Nicole, Alex and Maggie.
Our culture is still incredibly homophobic and hetronormative. When mainstream TV series do celebrate lesbians they can be amazing- but they are always pretty, skinny and pert: think Willow and Tara, Waverley and Nicole, Alex and Maggie.
The media does not celebrate young women who don’t want to play the patriarchy game. They are invisible. Think I’m exaggerating?
Try to think of a famous woman, a good role model for young women, who is a lesbian and doesn’t perform femininity. Most people are stumped.
Then they say “Oh, Ellen Degeneres!”
Degeneres is brilliant, charismatic and talented and has done a great deal to promote lesbian visibility; however she also fronts several ‘beauty campaigns’ as the face of Cover Girl make up and Olay ‘ageless foundation’.
So think again.

Big Boo – IKR
“What about Big Boo in Orange is the New Black?” someone once offered. Lea DeLaria who plays the character is a powerful actress and singer, but they weren’t referring to DeLaria. They were referring to Boo.
Think about that for a moment.
I asked someone to name a strong, gender non-conforming, lesbian role model and the best they could come up with was a prison inmate in an American sit com.
Are we surprised when some of these girls start thinking that maybe they’re boys?
Binding
 ‘Chest binding’, the action of wrapping ones breasts up so tightly that they become less visible, is popular among trans and non-binary-identified girls.
‘Chest binding’, the action of wrapping ones breasts up so tightly that they become less visible, is popular among trans and non-binary-identified girls.
A survey of 1,800 women who bound their breasts showed that 97% of respondents reported at least one negative outcome from binding. Surprisingly, commercial binders were the binding method most consistently associated with negative health outcomes. Young women who identify as trans or non-binary may bind using methods including from cling film and duct tape to wearing multiple too-tight sports bras.
We reject foot binding and chest ironing as barbaric practices, yet some schools enable this process of breast-crushing. Some UK schools have official policies to help girls in this endeavour. While acknowledging that binding ‘may even impair breathing‘, they suggest ‘short breaks could be offered discreetly’ to ease the discomfort of girls who want to bind their breasts. Even mainstream magazines like Cosmopolitan run articles on ‘how to do it’.
Some of the symptoms reported in the study mentioned above include: back pain, overheating, chest pain, shortness of breath, posture problems, itching, shoulder pains, rib fractures, spine problems, shoulder joint popping, numbness, headaches, fatigue, weakness, dizziness, heartburn, abdominal pain, muscle wasting, digestive issues, breast changes and tenderness, scarring, swelling, acne, coughs & respiratory infections.
You can read my article Bind Me here.
Autism
Bradley in conversation with Soh – see ‘podcasts’ at the end of this article for a link.
Austistic Spectrum Disorder studies in the UK suggest roughly 1% of the child population places somewhere on the autistic spectrum. In the USA approximately 1.7% of children are diagnosed with an ASD. Brugha’s 2009 survey of adults in England found that 1.8% of men and boys surveyed had a diagnosis of autism, compared to 0.2% of women and girls.
Yet almost HALF of trans-identified children seen by GIDS in the UK are on the autistic spectrum.
“Between April 2011 and August 2018, 48% of children and young people who were seen in GIDS and whose parents completed the social responsiveness scale (SRS), a quantitative measure of autistic behaviours in children and young people, scored in the mild to severe range” report Clarke and Spiliadis of the GIDS.
As Jane Galloway observes in her article ‘Autistic Girls, Gender’s Silent Frontier‘:
‘If there was any other connective factor affecting nearly 50% of all children referred to a particular service, there would be huge national interest and attendant press coverage.‘
“Adolescents by definition, have very little filter, no long term outlook, and a gigantic desire to have their desires indulged right now;” observes Galloway, “not because they are spoilt, but because impulse control and delayed gratification are far off distant concepts when you are a teenager.”
If a child doesn’t ‘feel like a girl’ then it may seem a logical progression to conclude that she must be a boy. Trans-lobby groups guidance does not addresses the issue of autism beyond suggesting trans-identified autistic children may need to have transition options explained to them more carefully.
The ‘Autism Speaks‘ website suggests that encouraging health providers to “use preferred pronouns during an office visit can go a long way toward establishing trust with your (undiagnosed, trans-identified, autistic) child.” Yet many critics feel that the affirmation model may be particularly damaging to autistic children.
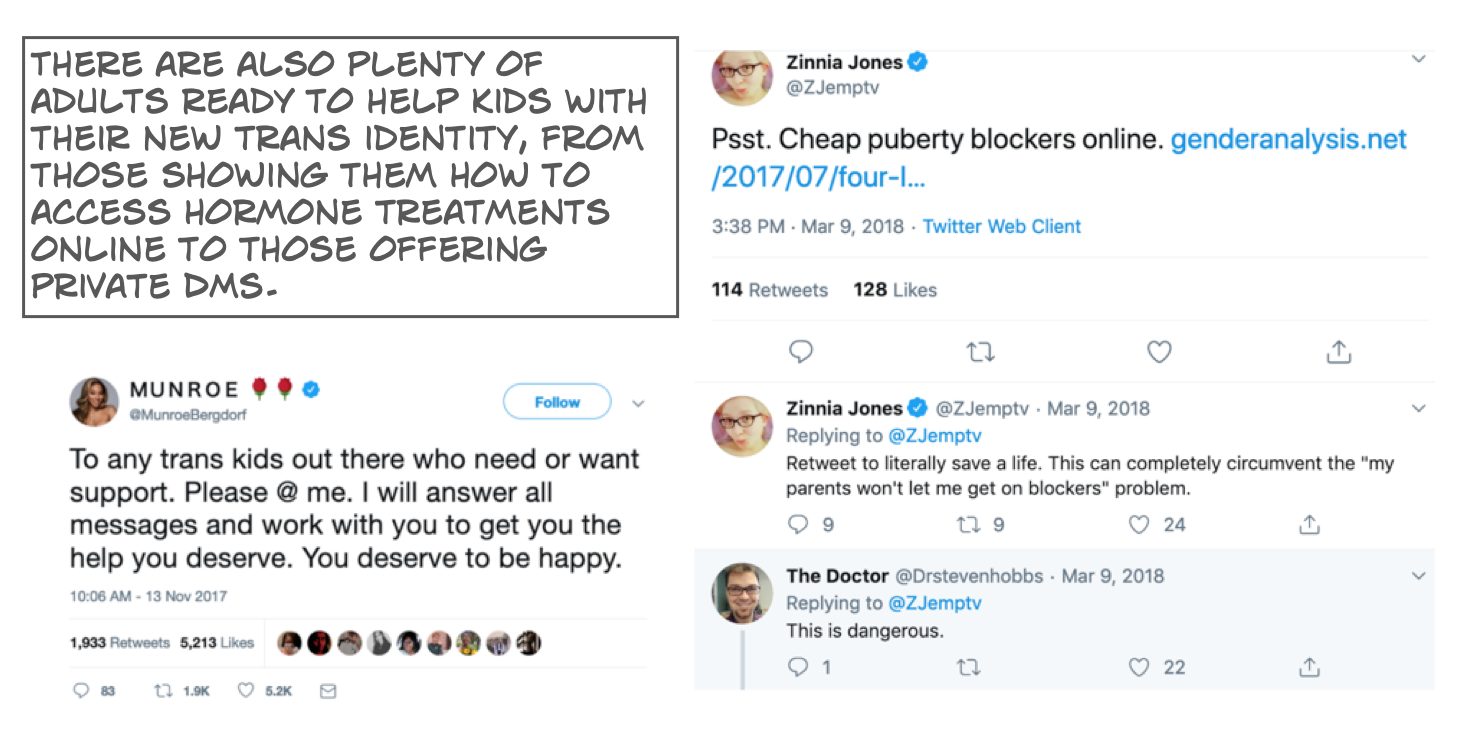
Physical transition
In the UK surgeries are not performed on children under the age of 18, and NHS gender clinics have long waiting lists. However, those who are willing to pay privately can access hormones and surgery with relative ease. In the USA and Canada girls as young as 13 have had their breasts removed. Complications with the coyly named ‘top surgery’ are not infrequent. Testosterone has been privately prescribed to girls as young as 12 in the UK. Susie Green, CEO and figurehead of the UK charity ‘Mermaids’ took her child to Thailand where, on his 16th birthday, his male genitalia were crafted into a semblance of a vagina. The minimum age for this operation was changed to eighteen shortly afterwards (the two events were unrelated).
Trans ‘support’ groups in the UK advocate not only for social transition but claim that some of these medical interventions are harmless or reversible.
Susie Green gives out mixed messages on this issue. In 2016 she tweeted “between your ears needs match what’s between your legs. Not your choice.” She has also told newspapers, “Medical intervention is very important, especially for teenagers who are already in puberty. It’s absolutely vital.”
Yet Mermaids claims to support both ‘trans and gender diverse’ children and according to an Independent article of December 2018, ‘primarily exists to support the families of trans and gender non-conforming children, not to coordinate their transition. It has no agenda.’
 Dr Norman Spack, a paediatric endocrinologist at the Boston Children’s Hospital (USA), who treated Green’s child, has prescribed puberty blockers to ‘about 200 children’.
Dr Norman Spack, a paediatric endocrinologist at the Boston Children’s Hospital (USA), who treated Green’s child, has prescribed puberty blockers to ‘about 200 children’.
He believes trans-identified children should be given blockers at the start of puberty, moving on to ‘sex-change’ hormones and surgery. He claims all of these 200 children have moved on to hormones and that ‘no one changes their mind’. He also recognises one of the more disturbing side effects of this combination:
“When young people halt their puberty before their bodies have developed, and then take cross-hormones for a few years, they’ll probably be infertile.“
“We don’t reassign a person’s gender,” he told The Guardian, in another interview, “we just acknowledge what it really is and fix it.”
Do these children really need ‘fixing’?
Remember that under the pre-affirmation model of ‘watchful waiting’ guidelines, around 80% of young people have desisted. It is not such a stretch of the imagination to consider that perhaps an affirmation model – with or without drugs- may be playing a part in fixing the idea of being ‘in the wrong body’ in children’s heads.
 Currently around 40% of children seen by the GIDS service go on to take puberty blockers. These drugs are used ‘off label’ and have been linked to problems with bone density. Almost all children who start on puberty blockers go on to take cross-sex hormones. The combination of the two is a recipe for sterile and inorgasmic young people.
Currently around 40% of children seen by the GIDS service go on to take puberty blockers. These drugs are used ‘off label’ and have been linked to problems with bone density. Almost all children who start on puberty blockers go on to take cross-sex hormones. The combination of the two is a recipe for sterile and inorgasmic young people.
“You could be the most transgender friendly service in the world and you would still have to consider some very, very grave issues. The timing of puberty suspension, for instance. Whether they can tolerate enough treatment to develop the lower part of the body so they develop physical sensations.” Bernadette Wren, GIDS
“Transgender youth may be interested in becoming biological parents, and should be counseled about potential risk of fertility impairment and fertility preservation options before initiation of hormonal or surgical therapies which may impact reproductive potential.” reports the Journal of Paediatrics in an article entitled ‘Understudied and Under-Reported: Fertility Issues in Transgender Youth’.
Dr Michael Biggs, an associate professor at Oxford’s Department of Sociology, has carried out research that suggests that puberty blockers can increase suicidal feelings; after a year of treatment a significant increase was found in female patients self-reporting to staff that they “deliberately try to hurt or kill myself”. Parents also reported “a significant increase in behavioural and emotional problems” and a “significant decrease in physical wellbeing” in these children after a year on medication, he told the Telegraph.
 At the WPATH Symposium in Amsterdam in 2016, GIDS (UK) reported statistics showing that children put on puberty blockers did not desist, as opposed to children not put on blockers, of whom 90% desisted.
At the WPATH Symposium in Amsterdam in 2016, GIDS (UK) reported statistics showing that children put on puberty blockers did not desist, as opposed to children not put on blockers, of whom 90% desisted.
The same report said children felt ‘happy and more confident‘ in the first six months on blockers, but after a year reported ‘an increase in internalising problems and body dissatisfaction, especially natal girls’.
“We have shifted to make the treatment (puberty blockers) available earlier and earlier,” Bernadette Wren of GIDS is quoted as saying in The Guardian. “But the earlier you do it, the more you run the risk that it’s an intervention people would say yes to at a young age, but perhaps would not be so happy with when they move into their later adulthood.”
The potential medical complications involved with ‘gender reassignment surgery’ (GRS) are multitudinous. The procedures- for example ‘skinning’ a female arm or thigh to create a roll of flesh which is attached between the legs to mimic a flaccid penis- are complex and the results are not always as desired. A boy moves from puberty blockers to cross-sex hormones and then desires vaginoplasty as a young adult, his pre-pubescent penis may not provide enough skin to create the neo-vagina and portions of gut may have to be used.
In one ‘phalloplasty regret‘ video on YouTube, a phalloplasty recipient tells viewers “There’s no erectile ability, there’s no ability to urinate, it’s basically just a piece of tissue sitting there.”
A Swedish study from 2011 suggested that “Persons with transsexualism, after sex reassignment, have considerably higher risks for mortality, suicidal behaviour, and psychiatric morbidity than the general population.”
Detransition

Desister Charlie Evans, who has written and spoken about her struggle with gender dysphoria.
There are a growing number of young people, primarily young women, talking about desistance (stopping a social transition) and detransition (stopping a physical transition).
Desister Charlie Evans has recently co-founded the Detransition Advocacy Network in England. Their website is currently under construction. You can read more about it here.

The Pique Resilience Project
The Pique Resilience Project is a ‘collective of detransitioned & desisted women igniting inspired and nuanced conversation that empowers’. All four young women experienced ROGD ‘and subsequently identified as trans men for several of our teenage years. We have all since detransitioned/desisted, and have been able to explore other individual factors that may have caused or exacerbated our dysphoria.”
PART TWO of this article (coming soon) will link to useful groups, resources, articles, studies, videos and podcasts.
Think of it as a little library….


Thank you for writing about this.
This is a wonderful resource – thank you
Pingback: So your child thinks they might be transgender? Resources for parents - Lily MaynardLily Maynard
Thanks so much for a comprehensive magazine style resource for frightened parents like us, with an autistic adult child caught up in “trans” social contagion.
Jeez, you really are taking things to an extreme. Gender clinics do not blithely hand hormones away to every child questioning their gender identity. There are loooong and involved processes to be gone through, and lots and lots of hoops to jump through to make sure that people like your daughter are not swept up with actual trans kids. Nothing bad would have happened if you had given your daughter access to medical help. In fact, she may have realised she was not in fact transgender sooner, and learned on the way that you would support her whoever she was and accompany her through all of her challenges in life, even if they did not conform to your expectations – something every child deserves from their parents. INstead, you have used the fact that your child has had a phase to fear monger to other parents and to strongly encourage (and yes, you are doing this, despite your attestations that you arent telling anyone what to do) people to oppose thier kids. Give your daughter some trust! And give the professionals involved some respect too – they do work with people who are questioning and going through phases as well as actual trans kids and the vast majority of them (just like in other medical professions) are doing a brilliant job. Always ask questions – I would say this for any medical process. Healthy skepticism is great. But that does not mean that opposing consensus is right for eveyone.
Your daughter seserved to be taken seriously and trusted to go thorough her process of exploration with your support, not resistance. She wouls have found her way through anyway.
It is possible for a 17 year old to get a prescription for hormones after one £200 appointment. Or parents can buy them off the internet. If I had purchased hormones for my daughter-as some parents do- she would have happily taken them. She has told me that. She has said ‘thank God you didn’t affirm me’on more than one occassion. You are obviously highly invested in your own child being trans (as you mention in one of your other comments). I wish them luck.
You are confusing buying medication for your child from the internet with affirmation and support from you. “It is possible for a 17 year old to get a prescription for hormones after one £200 appointment” is also misleading as it descibes someone elses ecperience based on their circumstances and need (some 17 year olds may be consulting help very late in the day and have become desperate by this point in tiime and prescribing quickly can be lifesaving). Otherwise, I am aware that privqate providers do exist where you can ‘buy’ an opinion and outcome, but I think its pretty clear that neither this, nor buying from the internet, is what I am talking about. The fact your daughter ‘would have taken’ hormones is neither here nor there as you’ve already established she was in a state of confusion and distress. Unconditional parental love and support with input, guidance and support from experienced professionals still seems to me like what’s called for.
“You are obviously highly invested in your own child being trans (as you mention in one of your other comments)” is a pretty strange conclusion to draw from this post (which does not even mentnion my child) and I can’t see where you’re getting the information to support this cheap tactic, presumably designed to make it seem as though my whole perspective stems from being ‘invested’ in my child being transgender. I am deeply ‘inested’ in both of my children’s wellbeing, and in fully supporting them regardless of whether or not either of them are transgender. My interest in anti-bigotry, including towards transgender people, predates me having children, as does my belief that supportive parenting is by far healthier than judgemental parenting and conditional love. I have had transgender people in my life consistently since I was a teenager and have transgender friends, colleagues and extended family (ie not including my child) and being transgender has never felt wrong or ‘unnatural’ to me. Nor do I put these friends, colleagues, family members on any kind of pedestal – they are people with all their full spectrum of qualities, just like my gender normative friends. I have, however seen how damaging the kind of bigotry you promote is to these loved ones and I dearly wish you would STOP perpetuating and promoting such hate and harm.
In terms of my own child, who is young. I am fully aware that this may be something that is grown out of, though it has been quite a long time now (early presentation and persisting for years) so, realistically, this is less likely as time goes on. In any case, it is who my child is now and there is no way I am going to reject who my child is right now.
But, to be perfectly honest and perfectly clear, had I had the option to wave a magic wand and made it all ‘go away’ so my child would not have to deal with walking the more difficult path of being transgender, yet be otherwised completely unchanged (ie to remain completely themselves), then this would have felt like a relief – not because I felt any rejection or discomfort towards my child identifying as a different gender from the one we had thought they were, and certainly not becasue there is anything wrong with being transgender (there absolutely is not), but becasue the anti-trans hatred, bigotry, discrimination and stigmatisation – that you are actively contributing to and spreading on this website – make it a very hard and very dangerous path to walk.
It is this hatred and bigoty and stigmatisation that means my child is statistically at dramatically increased risk of mental health problems and suicide just becasue of being transgender, and this terrifies me. It is my job to do everything I can to reduce this risk and fortunately there is a lot that I can do, as love, total acceptance, and support from parents already reduces it massively. As does that from siblings, extended family and friends. And as does that from a supportive community. Transgender people who are at most risk of suicide are those who have not come out yet and who, due the extreme lack of acceptance or support they’re surrounded by, are instead living repressed? Bigotry, hatred, stigmatisation and discrimination casues these risk factors and they go down as bigotry, hatred, stigmatisation and discrimination go down and go away if these go away, replaced instead by full and broad spectrum acceptance and support. This is why I am bothering to spend my already very stretched time writing to you and your forum.
I hope that some of the people who have found this forum while seeking out understanding for their own situations can listen to and take oon board what I am saying, whether you are here as parents, concerned loved ones, or interested individuals. Any change towards accaptance and support makes a big – and potentially life saving – difference to real individual’s lives (including your child or loved one if that’s why you’re here) as well as towards reducing the hate and bigotry trans people face en masse throughout their lives. So I hope you can listen, seek out further information and different perspectives, and find a way through.
Lily Maynard, it is evident from this website that you personally are too invested in your own anti-trans agenda to be able to even look at or acknowledge, let alone consider, anything that challenges it. You show this in the way you twist everything to fit what you’ve already decided, unabashedly use evidence seeking and confirmation bias throughout your website. So I recognise I am unlikely to change your mind. However, I still hope one day you will reconsider, and stop spreading dangerous hate.
I believe that transitioning children is child abuse & long term studies now suggest it is unlikely to be a solution to underlying mental health issues. I’m sorry you’re unable to see that rejecting the idea that your child is in the wrong body is not the same thing as rejecting your child. Despite your accusations of ‘anti-trans hatred & bigotry’, I’m approving your comment. I hope it all works out ok for you & your kids.
Do you seriously beleive that, had you taken her for professional help, the outcome for your daughter would have been a mistaken gender reasignement? This is ridiculous! Don’t you have any respect for your child at all?
As you have said, your daughter ultimately came to the conclusion that she is female and that “it was a decision she came to on her own after a lot of soul searching.” It sounds like it was a challenging time for her, and that her questioning and uncertainty were genuine at the time. Don’t you think that she would havew had a better time of it – and felt less alone in grappling with her soul – if she had had your full support and access to professional support as well? These professional see a lot of people who are ultimately just questioning and don’t turn out to be trans at all. In some cases children are confused in other areas of their lives – you dwell on sexuality, but there are lots of internal and external preassures of coming of age, and many ways other than homsexuality (which has extremely broad social acceptance now) that someone may be feeling ‘othered’, different, alienated or like they don’t fit in a way that is important to them). And yes, questioning their gender can be a way that children or young adults use to work through these feelings or stressors, sometimes ‘trying on’ another gender and even convincing themselves that it fits for a period of time before realising that it is not the issue after all – sublimating one thing into another is something that even adults do, and youth even more so. But, as you say, this is not an ‘end point’ for many people, and that is what your daughter had to work out all by herself, and even amidst the added confusion and confabulation that the resistance that you yourself have said you contributed as added into the mix of thoughts and feelings to work for.
What strikes me is the disdain and extremely low esteem you give to the professionals who could have offered her support – including specialised psychiatrists and psychologists as well as an array of other experienced professionals . Do you really beleive that the only input they would have had would be to shove hormones in her direction and send her packing, all set to transform into Jak whether that’s what’s right for her or not? A kind of wham b’am thank you sirma’am approach to gender reassignment? Your level of underestimation of the sensitivity, tenacity, dedication and expertise of the professionals involved is staggering!
These professionals are used to people in your daughters situation, just as they are used to working with genuine trqansgender children and young people. And they are very, very used to helping people work through what is really going on with them. They would have helped her when she needed it most and she would not have had to do all the work alone, with the only input being resistance/rejection from her mother to what she at the time genuinely appears to have beleived to be her true self. Do you really beleive that that maternal rejection helped her? Do you really not see that it was just another pressure put on her to be something that at that time she clearly beleived she couldn’t be, at least in the way she understood it and how she was feeling then. Do you really beleive that professional help would not have hlped her find clarity sooner, and ideally also identify what it is/was that she was actually struggling that sent her down this path of exploration in the first place.
Yes, detransition does happen. But is is very, very, very rare. In the scheme of misdiagnoses accross the medical spectrum, or mis-instructred medical intervention, it is strikingly rare. Look at the statistics. Even not going by statistics but by anecdotal evidence (as you seem to prefer), everyone knows multiple people who have been medically misdiagnosed or who have had medical interventions that turned out to be unnnecessary or even harmful – in my family, for example, there is myself (multiple cases of misdiagnosis, one count of unnecessary surgery, and while pregnant with my second child and suffering a medical emergency I had to repeatedly state ‘I do not consent’ whilst going in and out of consciousness in order to stop my child being aborted, which is what the doctors wanted to do and which would have killed us both, then theres my my father (2 counts of harmful and unneccessary surgery, 3 counts of misdiagnosis), my eldest child at birth (dangerous misdiagnosis – risked her life), then to greater or lesser extents, my brother, aunts, uncle, neices, and nephew and cousins. In fact at least half of my parents and my generation of my family has had major medical misdiagnosis or incorrect/harmful treatment impact or threaten our lives. I have to assume we are higher than the average, but I would bet you know at least several people who have had at least a significant misdiagnosis. In the face of this, the amount of people who have gender reasignment who actually don’t need it is absolutely microscopic. It is the lowest error percentage of any medical specialism I can think of by a huge margin.
So why are you fluffing it up to be a huge risk? Hmmmm, let me think… could it be prejudice (presumably fuelled by genuine good intentions but underlying ignorance and bias)? Or is it straight out fearmongering for the sake of it, even after knowing that you are creating an allusion of threat where there is none. I really hope it is the former. And I really hope you can get to grips with it before you do more damage.
There’s no such thing as a transgender child.
You are adding to this:
“According to official government figures, transphobic hate crimes rose by 56% during 2022 – transgender hate crime figures have been rising year on year since 2009, and have quadrupled in the last 5 years”
and:
“Stonewall’s 2017 schools report suggested that 64% of trans pupils experience bullying at school, with 1 in 10 being subjected to death threats”
Do you really want to contribute to this kind of hate in the world? Becasue right here, right now, that is exactly what you are doing.
(source: https://hackney.gov.uk/equal-gender-reassignment/#census)
STOP, THINK, CARE, and decide instead to become a pert of this:
“Just Like Us’s 2021 research suggests pupils in schools with strong positive messaging about being LGBT+ have drastically improved wellbeing and feel safer – regardless of whether they are LGBT+ or not.”
Choose to be a force for good in the world. Or at the very least, please STOP preaching hate!!!