
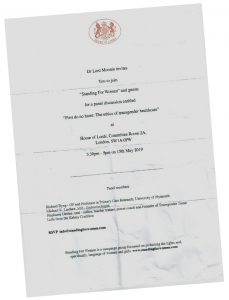
The House of Lords played host to a series of short lectures on transgender healthcare on 15th May 2019. Controversy, no surprise, raised its head before the lectures began.
The event was organised by ‘Standing for Women‘ and sponsored by Lord Moonie, ex-Defence Minister, psychiatrist, medical expert and life peer.
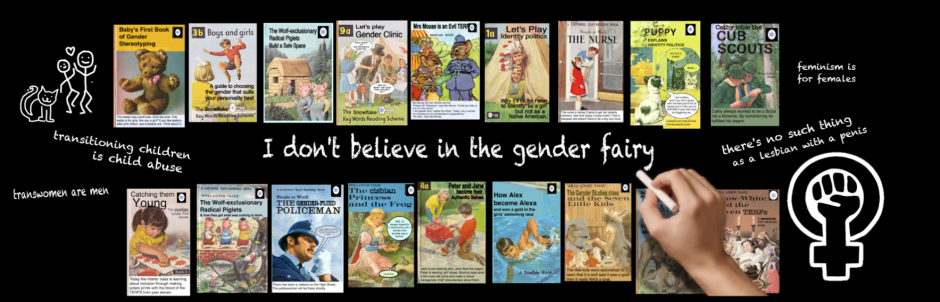
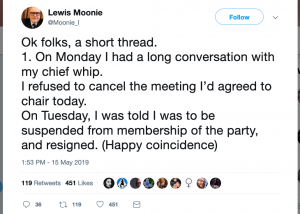 Lord Moonie resigned from the Labour Party the day before the meeting. He was suspended for investigation into ‘transphobic’ Tweets, including the observation: “Trans women are and remain men. No less valid as individuals, just not women. Ever.”
Lord Moonie resigned from the Labour Party the day before the meeting. He was suspended for investigation into ‘transphobic’ Tweets, including the observation: “Trans women are and remain men. No less valid as individuals, just not women. Ever.”

Lord Moonie sponsored the meeting because, he says “I am concerned about the growing number of individuals, especially children, who are being diagnosed with gender dysphoria and with the treatment that is currently available to them… we are duty bound to question any new treatment protocols that do not have proven outcomes.”
I know his reasons, not because I have a photographic memory or psychic powers, but because those of us who attended the meeting were given a copy of ‘Duty of Care – First Do No Harm – the ethics of transgender healthcare’, a high-content, high-quality booklet produced by Standing for Women, containing some details of the lectures given by each attendee and a short introduction by Lord Moonie himself.
 Here I’ve tried to capture the essence of what the speakers said that day, the response of David Bell to Lord Moonie’s suggestion that he might like to ‘add a few words’ and the discussion that ensued after the panelists had spoken. Transcripts of some of the full scripts are available here at the Transgender Trend website, and the booklet given to attendees can be purchased from Standing for Women.
Here I’ve tried to capture the essence of what the speakers said that day, the response of David Bell to Lord Moonie’s suggestion that he might like to ‘add a few words’ and the discussion that ensued after the panelists had spoken. Transcripts of some of the full scripts are available here at the Transgender Trend website, and the booklet given to attendees can be purchased from Standing for Women.
Got a cup of coffee and a packet of oreos on hand? Good.
 Surfacing from the underground at Westminster, I scuttled past the BREXIT protestors, collected my name tag and cleared security into the Houses of Parliament. Passing through St Steven’s Hall I took a moment to catch my breath and admire the great window. Up the stairs, along the hall lined with marble statues of dead, white men -all be-wigged and delicately shod – I finally arrived outside Committee Room, a few minutes late. Not so late as to have missed very much, but just late enough to be embarrassing.
Surfacing from the underground at Westminster, I scuttled past the BREXIT protestors, collected my name tag and cleared security into the Houses of Parliament. Passing through St Steven’s Hall I took a moment to catch my breath and admire the great window. Up the stairs, along the hall lined with marble statues of dead, white men -all be-wigged and delicately shod – I finally arrived outside Committee Room, a few minutes late. Not so late as to have missed very much, but just late enough to be embarrassing.
The room was not enormous, but it was absolutely packed and somewhat stuffy. I squeezed in at the back and wrestled myself out of my coat, like a captive octopus, trying not to bump into the women on either side of me. Perching my notebook on my lap, I fumbled in my handbag for my pen.
After Lord Moonie’s introduction, the first speaker was Richard Byng.
Richard Byng
A GP, and professor in Primary Care Research at University of Plymouth, Byng specialises in ‘the development and evaluation of complex interventions for marginalised groups and those with mental health problems’. He is concerned about the harm that may be caused to vulnerable young people via untested, inappropriate or hasty treatments. It was his first time speaking on this ‘very contentious‘ subject.
Byng regularly encounters young people who are questioning their gender. Many are dissatisfied by the failure of medicine to adequately increase beard growth or redistribute body fat or by feelings of sexual inadequacy. Some of these young people ‘don’t necessarily want to transition but feel they might be trans’. Byng is strongly aware of the polarisation of postions and perceives the basis of different opinions among doctors to be founded on three main areas of belief.
First, he told us, is the understanding of brain, body and mind and how this affects our decision making. Medicine usually sees sex as binary and fixed, but queer theory believes the individual’s views on their gender is the most important thing; that people can be ‘born in the wrong body’ and that medical intervention should follow. This, Byng believes, does not give patients the ‘inquisitive, compassionate, but neutrally framed support’ that doctors should be providing.
 Secondly, Byng observed that there’s a difference between informed consent and the ‘purely consumerist’ approach of giving people whatever medicine they ask for. Options, and the uncertain risks of treatment may not always be fully discussed with young people, and this can result in harm.
Secondly, Byng observed that there’s a difference between informed consent and the ‘purely consumerist’ approach of giving people whatever medicine they ask for. Options, and the uncertain risks of treatment may not always be fully discussed with young people, and this can result in harm.
Thirdly, a small group of ‘dedicated gender specialists’, doctors with limited resources, have generated a body of evidence concerning medical intervention and medical techniques. ‘This is in many ways impressive, asserted Byng, but lacks the normal requirement of evidence. There have been few trials, they are small scale, short and without follow up.
Byng quotes Oxford University’s Carl Heneghan, who says,“current evidence does not support informed decision making and safe practice.”
These three issues: overselling of benefit, unscientific thinking and a consumerist approach, along with cultural changes, have led to the current situation.
 Byng is especially concerned about the harms of applying ‘a relatively poor evidence base’ to a new and growing group of young, mainly female, individuals, many of whom present with ROGD, past trauma and/or autistic traits. He also believes that provision for 17-25 year olds under new NHS adult services will not provide enough psychological assessment. Many issues need to be considered when dealing with young people with gender dysphoria, and both transition and detransition may result in short and long term physical side effects, emotional problems and social difficulties.
Byng is especially concerned about the harms of applying ‘a relatively poor evidence base’ to a new and growing group of young, mainly female, individuals, many of whom present with ROGD, past trauma and/or autistic traits. He also believes that provision for 17-25 year olds under new NHS adult services will not provide enough psychological assessment. Many issues need to be considered when dealing with young people with gender dysphoria, and both transition and detransition may result in short and long term physical side effects, emotional problems and social difficulties.
Byng suggested that to ‘create the best service in the world for gender questioning individuals’ we needed to do the following.
“All medical and surgical interventions for those under 25… should be halted, except under research conditions, with randomised controls and independent monitoring. Instead we should provide compassionate, person-centred, psycho-social support.”
He also believes that such a change is unlikely in the immediate future and that harms can be lessened by the following:
Prevention: A ‘complex mix of cultural norms and personal predispositions’ result in trans feelings. Schools especially need to stop encouraging individuals to see themselves as ‘trans’ and ask why so many girls feel uncomfortable or disgusted by their bodies.
Providing accurate information: We must stop glamourising sexual stereotypes and transition. NHS and other websites need to mention potential harms as well as benefits.
Adopting a person-centred and scientific approach, as mentioned above.
Offering ‘neutrally framed support’ individuals to help them come to terms with their biological bodies: this includes psychological support for 17-25 year olds, acknowledgement that some people will desist or detransition and services for those that do.
Finally, Byng recommended bringing together GIDS and adult services in ‘an ongoing long-term cohort research study’.
Marcus Evans
Dr Evans worked in psychiatry for many years and was part of the Tavistock management group for 20 years, retiring in Easter 2018 and taking up a post as governor, before resigning over concerns about how the Trust dealt with both Dr Bell’s report (see below) and over a letter from a group of parents whose children were being treated by the GIDS service.
Dr Bell, a senior consultant and governor, had been approached by ten staff members who had ‘grave ethical concerns’ – complaining of inadequate assessments and the influences of trans pressure lobbies – and a letter from a group of parents who felt their children were being ‘fast tracked’ to medical interventions.
The Trust, in response, asked the medical director to conduct a review. Trust management, Evans claims, dismissed and undermined these concerns and questioned the validity of Dr Bells’ report. He believes that such behaviour ‘is often driven by a defensive wish to prevent examination of an over-valued system‘ and is especially worried as the GIDS service is treating vulnerable individuals & families.
 Evans’ own research and experience, over 40 years, suggests that the positive outcomes promoted as linked with transition are not always the case. In the 80s he assessed adult parasuicides at Kings Hospital, and several had undergone GRS. Often they were unhappy with inadequate psychiatric services and ‘angry at their loss of biological sexual functioning’. He has also encountered patients with serious or long lasting mental disorders who had developed late-onset GID, undergone GRS and found it did not solve their problems. In fact, ‘self-harming and suicidal tendencies escalated’.
Evans’ own research and experience, over 40 years, suggests that the positive outcomes promoted as linked with transition are not always the case. In the 80s he assessed adult parasuicides at Kings Hospital, and several had undergone GRS. Often they were unhappy with inadequate psychiatric services and ‘angry at their loss of biological sexual functioning’. He has also encountered patients with serious or long lasting mental disorders who had developed late-onset GID, undergone GRS and found it did not solve their problems. In fact, ‘self-harming and suicidal tendencies escalated’.
‘Adolescence’ he continued, ‘ is a developmental process and all individuals experiment with different identifications, including male and female ones‘ which can result in confusion, doubts and conflicts. Feelings of being ‘dislocated from one’s changing body’ are not uncommon in adolescence and it is essential to tolerate these confusions and avoid early transition. However, the gender dysphoric person and their family often put a great deal of pressure on clinical services ‘to provide the medical intervention that they believe will cure the dysphoria’ and get rid of the confusion. This is exacerbated by the long waiting lists which can be as long as two years and often leave patients arriving at the service ‘in a really bad state‘.
‘In this way, a psychological prang’ is treated as if it were a concrete problem located in the body.’
 Evans referred to a case where the Chief Executive of the Tavistock told a parent that gender dysphoria was not a psychiatric condition and had to be corrected by them. The idea that it is not, Evans points out, is often promoted by pro-trans lobbies, who suggest there isn’t any psychological disturbance underlying the patient’s thinking.
Evans referred to a case where the Chief Executive of the Tavistock told a parent that gender dysphoria was not a psychiatric condition and had to be corrected by them. The idea that it is not, Evans points out, is often promoted by pro-trans lobbies, who suggest there isn’t any psychological disturbance underlying the patient’s thinking.
Evans also emphasised the importance of acknowledging that it is not possible for someone to ‘entirely eradicate the biological realities of natal birth’. For this reason, psychological work is extremely important.
Anonymous clinicians have claimed that this process is not followed at the Tavistock, partly due to pressure by pro-trans lobby groups. Young people, he says, should not become the symbol of a political group. Examining different points of view is difficult in the current environment, when accusations of hate speech or transphobia shut down the thoughtful inquiry that is needed ‘so we can protect children from being harmed.’
Michael K Laidlaw
Endocrynologist Laidlaw thanked Posie and Venice for inviting him and said it was ‘a great honour to be here’. There were, he said, three questions he wanted to address and answer.
Is a person born a man or a woman?
Neither. A person is born as a girl or a boy. Although this may seem obvious, it is important. While hearts and kidneys are born fully functioning, the testicles and ovaries are not: they await a signal from the brain. Puberty can occur around the age 0f nine and is divided into five ‘Tanner’ stages. Fertility is established around stage four, and stage five is normal adult development.
What happens to a child when normal puberty is blocked?
 Problems with the pituitary gland can be treated by endocrinologists to enable normal development. The process of stopping the development of puberty can also be undertaken by endocrinologists – and gender clinics throughout the world, including the UK, are prescribing these problematic medications to children. Sexual organs are not developed at birth and stopping puberty at stage two results in sexual dysfunction.
Problems with the pituitary gland can be treated by endocrinologists to enable normal development. The process of stopping the development of puberty can also be undertaken by endocrinologists – and gender clinics throughout the world, including the UK, are prescribing these problematic medications to children. Sexual organs are not developed at birth and stopping puberty at stage two results in sexual dysfunction.
The final stage of surgery for trans-identified youth is to have testicles or ovaries removed and this leads to complete sterility and sexual dysfunction. Given that blockers are administered to children as young as age eight, Laidlaw asks if these children really have the capacity to give informed consent and understand the consequences of these medications?
 Next he asks if these medications really do help the gender confused child. Professor Michael Biggs of Oxford University found, through a Freedom of Information Act request to the Tavistock, that they do not. Unsurprising in the light that these medications are labelled with warnings to ‘monitor for development or worsening of psychiatric symptoms.’
Next he asks if these medications really do help the gender confused child. Professor Michael Biggs of Oxford University found, through a Freedom of Information Act request to the Tavistock, that they do not. Unsurprising in the light that these medications are labelled with warnings to ‘monitor for development or worsening of psychiatric symptoms.’
Do we have the technology to turn a boy into a woman or a girl into a man?
Cross sex hormones are being given to youths and adults in doses 10-40 times higher than upper limit of normal range for testosterone, and double or triple normal levels for oestrogen. Risk of deadly blood clots in males is increased five times. Females have an increased risk of both breast and ovarian cancer. Both males and females are at higher risk of cardio-vascular disease. Yet the American Society of Paediatrics suggests children should receive these treatment based solely on self-identification, ignoring the ‘watchful waiting’ worldwide standard of care.
The Swedish National Council on Medical Ethics (April 2019) concluded that treatment recommendations for gender dysphoria in children and youth must be revised as soon as possible. The Swedish Paediatrics Society stated that ‘giving children the right to independently make vital decisions… is not scientifically founded and is contrary to medical practice’.
The editor in chief of the British Medical Journal came to the conclusion that current studies were not evidence based, calling puberty blocking treatments ‘a momentous step in the dark‘. There is a lack of quality short term studies and no long term studies on the effect of these treatments for young people.
“Mary Shelley quotes Milton in the chapter of her famous novel,” concluded Laidlaw.
“Did I request thee, Maker, from my clay / To mould me Man, did I solicit thee / From darkness to promote me?”
This quote takes on a new significance when a man wants to be made woman, or a girl wants the impossibility of becoming a man. Some suggest children should have access to medications and surgeries from any age to allow them some semblance of becoming the opposite sex and wish to pass laws to help this happen.
Laidlaw concluded, “It appears at this point in time that we are harming these vulnerable youths in so many more ways than we are helping.”
Leila Leoncavallo
 Leoncavallo has degrees in Psychology and Law and is founder of Fairfax Dyslexia. She was admitted to the Virgina State Bar in 1994. She is a member of Phi Beta Kappa and lectures weekly at the US Supreme Court.
Leoncavallo has degrees in Psychology and Law and is founder of Fairfax Dyslexia. She was admitted to the Virgina State Bar in 1994. She is a member of Phi Beta Kappa and lectures weekly at the US Supreme Court.
Beginning by thanking us all for being there to hear about the ‘importance and urgency of this issue’, Leoncavallo said she was here to represent the Kelsey Coalition and the voices of ‘powerless parents’.
Referring to the huge surge in trans-identified children, she acknowledged ‘their feelings and pain are real, they should be treated with respect and compassionate care’ going on to add that this does not need to include immediate affirmation from teachers and therapists, resulting in ‘invasive, risky and poorly researched medicalisations’.
Teachers in some US schools, she said, teach children that sex is ‘assigned to them by a doctor’ but that they can choose whether to be a girl or a boy. The same teachers are told not to notify parents when their child changes name or pronouns.
She tells us the story of parents whose 13 year old daughter was diagnosed as transgender by a ‘prestigious gender clinic’ within just a few hours. The clinician’s recommendation? Start her on testosterone that very day.
The parent of a girl who began to think she was transgender aged 15, told Leoncavallo:
‘It is difficult for us to get any help other than from those who think she should pursue medical treatment.’
Other parents, who supported their daughter in cutting her hair and choosing new clothing, told her they ‘wanted to explore where these feelings were coming from, but everyone we consulted (including the child’s school and therapist) pushed unquestioning affirmation… all encouraged our daughter to move away from the support and love of her family.’
Another mother is quoted as saying, ‘I took (my daughter) to a gender therapist and was shocked to learn there was no test, no diagnosis, no criteria beyond a child’s feelings during puberty to verify whether or not her self-diagnosis was accurate.’ When she questioned this, the child’s mother was called transphobic by the therapist. The child, who had recently lost her father, was sent to a doctor who put her on puberty blockers at a first visit and testosterone on the third.
Young adults, asserts Leoncavallo, are perhaps more vulnerable to the machinations of unscrupulous practitioners. Informed consent clinics will provide hormones to young people without medical history or mental health assessments. Often, university health plans in the US will cover both hormones and surgeries.
“… at a second visit she received a prescription for testosterone,” tells one parent of their eighteen year old daughter’s experience.
Leoncavallo tells us several more stories of young people fast tracked into hormones and surgery, including a young man with terminal cancer who was prescribed ‘feminising hormone treatments’.
In Oregon, she reminds us, fifteen years olds can receive hormones and ever surgeries without parental permission. Money is no barrier because government funded MedicAid program will cover many of these ‘treatments’.
The story that affected me the most was that of a mother who reported that her ‘sweet, loving girl changed almost overnight’ after coming out as trans age fourteen. Her daughter was diagnosed with ADHD, depression and anxiety. Age sixteen, her daughter found an endocrinologist who taught her to inject herself with testosterone. Soon after, her daughter ran away to Oregon. The rest of her story was recorded in the booklet accompanying the talks:
“At the age of seventeen, without my consent or even knowledge, my daughter was able to change her name and gender in court, obtain testosterone treatment, a double mastectomy and a radial hysterectomy. Recently surgeons performed another irreversible and risky procedure, a radial forearm phalloplasty on my now 19 year old daughter. They removed part of her arm to surgically construct an imitation penis. My once beautiful daughter is now homeless, living in poverty, bearded, sterilised and extremely mentally ill, but not receiving any mental health services. She tells me that she is in constant pain.“
“I have met this heartbroken mother.” Leoncavallo tells us. “As incredible as her story is, I can promise you that it is true. I want to show you some pictures that her mother shared with me.”
We are shown pictures of a baby, a small child and an older child, smiling happily at the camera. Then we are shown a picture of the young woman at seventeen. She is posed lying across a bed, topless. She sports a bushy beard and surgery scars from her double mastectomy. She is wearing rainbow Y-fronts.
There is not a single long-term study to support the use of these interventions, concludes Leoncavallo. We must stop this.
Stephanie Davies-Arai
Davies-Arai has delivered courses and workshops for parents and schools for over twenty years and is the author of Communicating with Kids. In 2015 she founded Transgender Trend who released their schools packs in 2018. Her talk was titled ‘The spread of an ideology and the targeting of children in UK schools’.
Davies-Arai asserted that the huge rise in children presenting to the Tavistock Gender Identity Development Service must be seen within the context of “the current worldwide cultural obsession with ‘gender identity,’ driven by a global transgender activist movement.”
The groups providing transgender training to the NHS, police, prisons and teachers are not trained professionals but lobby groups, heavily funded by lottery and government grants. Groups such as Mermaids, GIRES and Gendered Intelligence wish to replace the reality of biological sex with ‘gender identity’, both legally and culturally, and advocate for the social transition of gender dysphoric children.
School children are taught, often with the aid of picture books and programs on children’s television, that sex is merely ‘assigned at birth’ and that exploration of their ‘innate gender identity’ will lead them to discover if they are really a boy or a girl.
This, says Davies-Arai, is ‘adult activism imposed on very small children’ and teachers are being led to believe they have to affirm these ideas.
Children are being groomed by activists on social media, where they learn the art of ‘mechanically repeating dogma’. They are told how to acquire hormones online and encouraged to use the threat of suicide to manipulate their parents. Children are being taught that if their parents disagree with this ideology they are transphobic and hateful. A child who believes themselves to be transgender is thus ‘placed outside safeguarding and outside parental protection, leaving them vulnerable to influence from external agencies’.
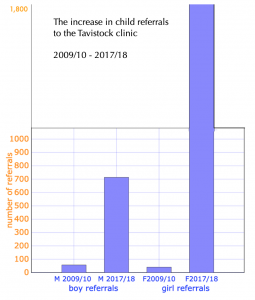 Davies-Arai pointed to the huge increase in child referrals to the Tavistock over the last decade: the increase is 1,173% in referrals of boys, and 4,415% increase in referrals of girls.
Davies-Arai pointed to the huge increase in child referrals to the Tavistock over the last decade: the increase is 1,173% in referrals of boys, and 4,415% increase in referrals of girls.
(Yes, you did read that right!)
Rapid onset of gender dysphoria (ROGD) in adolescent girls who have no history of gender dysphoria in childhood is ‘a newly-created phenomenon for this generation’ observed Davies-Arai. Historically transexuals have been predominantly autogynophilic men. Childhood-onset gender dysphoria was much rarer, and under a process of ‘watchful waiting’ only 20% of these children went on to transition. A majority grew up to be homosexual.
 Yet hormones- and puberty blockers which we know ‘virtually guarantee progression to cross-sex hormones‘- are now being given to ROGD teenagers.
Yet hormones- and puberty blockers which we know ‘virtually guarantee progression to cross-sex hormones‘- are now being given to ROGD teenagers.
“Unquestioning affirmation is not a neutral act of kindness, but an intervention that actively shapes and changes a child’s development.”
Daily affirmation from adults in positions of trust reinforces a child’s idea that they are actually the opposite sex. This changes a child’s neural pathways: social transition has been shown to affect persistence rates, leading young women who desist or detransition to ask “‘why did no-one tell me I could never actually be a boy?’
When a child’s body is cast as ‘an inconvenient mistake’ it leads to the child feeling contempt for their body and this puts children and their bodies at risk.
 Davies-Arai concluded by saying she has seen at first hand how the mental health problems of our most vulnerable young people are often made worse after ‘coming out’ as trans.
Davies-Arai concluded by saying she has seen at first hand how the mental health problems of our most vulnerable young people are often made worse after ‘coming out’ as trans.
“We must support children who identify as transgender in schools but we must not encourage children to understand their problems within this one prescribed conceptual framework.”
Children are being used as test subjects for ‘gender theory and queer theory’ and we need to start from a ‘basis of reality’ when dealing with children. We must protect children from lobby groups presenting ‘ideology masquerading as fact’ and ensure that young people have access to accurate information and a range of support services suited to their individual needs. This includes the 17-25 year old age group, which is particularly vulnerable and can ‘slip between the gaps between child and adult services‘. We need, concluded Davies-Arai, long term research with measured outcomes and proper follow up, and a review of the use of medication on young children.
“Those were very good presentations, thank you,” commented Lord Moonie. “Before I throw this open for general questions, David Bell is here and I wonder if he might like to add a few words?”
David Bell
Bell is the consultant psychiatrist who carried out the report of the gender service at the Tavistock. The report was leaked and is now in the public domain. He said that, as an employee of the Trust, he was limited in what he could say and that it was important to acknowledge that anything he did say was his own personal view and not necessarily the view of the Trust.
“Gender dysphoria,” he said “is a disturbance of state of mind arising from conflicts about gender. Transgender is a statement about a wish to change gender and an identity.” The difference is important and the complexity of the issue must not be underestimated.
The children who come to the Tavistock are ‘a disturbed population with multiple pathologies’ who may have suffered sexual abuse or been subject to homophobia. They may suffer from depression or ADHD. “Often they are children who are lost in the world.” Peer group pressure or online influences offer them a new identity and a ‘script’ to present parents and clinicians.
 The huge cuts in mental health services mean that if a clinician is able to put a child’s issues under the umbrella of ‘transgender’ the child can be sent to a specialist service. Thinking about these issues is being ‘peculiarly cast as transphobic’.
The huge cuts in mental health services mean that if a clinician is able to put a child’s issues under the umbrella of ‘transgender’ the child can be sent to a specialist service. Thinking about these issues is being ‘peculiarly cast as transphobic’.
He talked about how in the past gay men were given hormones and coercive therapy in order to change their identity. People who want to think about things, he reiterated, are those who want to stop conversion therapy. It’s important that we defend the right of trans people not to be discriminated against but it should not be confused with the need to affirm identity in children.
He believes that society’s increasing ‘idealisation of macho ideals’ feeds the misogyny that these young women experience; for some it is more about not wanting the body they have than actively desiring to be something else.
 The increase in numbers of children presenting to the Tavistock represents ‘a socio-cultural phenomena which we do not understand’.
The increase in numbers of children presenting to the Tavistock represents ‘a socio-cultural phenomena which we do not understand’.
The refusal to investigate and instead to treat reflects the change from patienthood to customer and the growth of identity politics.
Further Discussion
Audience members, including academics and lawyers spoke of the ‘climate of intimidation’ and how there are current cases concerning free speech on this issue.
It was suggested that forthcoming cases concerning medical negligence might leave lawyers as the only ones benefiting from the current situation. It was mentioned that a group of young women in the US had wanted to take legal action concerning their treatment but had been unable to get funding. In the UK there have been cases involving out of court civil settlements. It was also suggested that undiagnosed PTSD was an issue in many cases.
“What can we do,” asked James Caspian, “when even just sitting here discussing this would have us all labelled TERFs, transphobes, bigots, right-wing fundamentalists… that’s what happens. People are intimidated… most of the people speaking here have either resigned or are self-employed.”
David Davies echoed Caspian’s concerns and said after his last meeting in the Lords he was told by somebody in the Whips office that speaking out on this subject meant he would never get promotion.
A GP said, “All my colleagues find this issue incredibly problematic… I don’t know one GP who is at ease with this approach, it’s just sort of been dumped on us.”
Since when has questioning gender roles been an issue, she asked, adding that she was deeply concerned about young lesbians. So far she had refused to prescribe hormones or blockers and wondered if she could take the issue to the GMC. Another GP spoke about bridging hormones and how the GMC website did not make it clear that GPs did not have to prescribe them.
Julia Long pointed out that children learn from what they see around them, and as long as the adults around them are conforming to gender stereotypes and acting as if those stereotypes are real, children will copy us.
Several people commented on the influence of social media and others on the problems involved with confusing the ideas of gender and sex. It was observed that some families are not comfortable with homosexuality and might prefer to have a transgender child than a gay child.
A woman spoke about bullying and harassment in elite sport, how the rules concerning testosterone suppression had been changed, and how self-id was affecting young women’s scholarship positions. Tokyo will be the first Olympics where transwomen will compete and it is up to ex-atheletes to speak up about this. Stephanie replied that in schools in the UK girls were being called bigots if they didn’t want to compete against trans-identifed boys.
Heather Brunskell-Evans made the point that “‘it isn’t about gender freedom it’s about intensifying very old fashioned (patriarchal) ideas about gender… children are being used for political ideology and this is the very thing we can’t say… that there isn’t any such thing as a transgender child.”
Posie Parker wanted to know how parliamentarians could be persuaded to listen to reasonable voices. She told how she visited her MP and told him he needed to raise questions in parliament. “You’re my hope, you’re my voice to power. What hope have we got?” she had asked him. And her MP had replied “Well, we’ve got you.”
“We’ve got to take the long term view that we can change behaviour, and change the understanding of the issue, but it’s going to take time.” replied Lord Moonie.
“A lot of people just don’t realise what is happening,” said one audience member, “and a lot of people are worried about putting their heads above the parapet, even in this place.”
Maya Forstater, who was fired from her job for her views on gender, told how she is taking her employer to court over the protected characteristic of belief. People say ‘of course we must talk about this but I’m too scared.’ This has to change.
A parent spoke of losing contact with all of her children over gender ideology and because she couldn’t believe her children were not the sex they were born. “Parents are absolutely terrified.. they can get no doctor to help them.. no therapist to help them… there’s nowhere to go.”
“It’s very difficult for a clinician… to have the freedom to do their job. It isn’t my job to agree or disagree with the patient, it’s my job to think about the patient and open things out. We’re all complicated. It’s care that makes us behave thoughtfully and rigorously with our patients, it’s not hatred.”
“I see families torn apart by this,” added Davies-Arai, “It’s the most damaging phenomena I’ve ever seen and I’ve worked with parents for over twenty years… parents are painted as bigots and transphobes… and children are coached to do this online… parents report that it is as if their child has been taken over by a cult.”
In some states in the US, we were told, teachers are actively encouraged to report parents who do not affirm their children.
Sue Evans, who resigned from the Tavistock many years ago, raised the issue of James Caspian being closed down by a university for trying to study detransitioners. He needed, she said, to have freedom of speech to represent people who have been mistreated in the past.
David Bell pointed out that if a doctor had a patient who hated his arm, the doctor would try to reconcile that man to his healthy arm rather than remove it. Is that conversion therapy? Earlier he had told a story about helping a man who hated his ears reconcile with them and work, over a period of time, through the issues (in this case problems with his father who had similar ears) that had led him to feel that way. He pointed out the incongruence that a child who says he hates his penis is put on blockers.
 Journalist and film maker Sonia Poulton observed that the media is largely complicit in promoting trans ideology. Poulton recently appeared on This Morning, ostensibly to discuss the LGBT sandwich . After digressing onto the subject of the cotton ceiling, she mentioned she was making a film about trans issues and was later approached by several interested broadcasters and streaming services. This wouldn’t have happened two years ago, she professed. Editors and journalists have been petrified about speaking out of line but behind the scenes she believes things are changing.
Journalist and film maker Sonia Poulton observed that the media is largely complicit in promoting trans ideology. Poulton recently appeared on This Morning, ostensibly to discuss the LGBT sandwich . After digressing onto the subject of the cotton ceiling, she mentioned she was making a film about trans issues and was later approached by several interested broadcasters and streaming services. This wouldn’t have happened two years ago, she professed. Editors and journalists have been petrified about speaking out of line but behind the scenes she believes things are changing.
To much applause Stephanie Davies-Arai mentioned that the Transgender Trend schools pack had recently been voted ‘most compliant with EHRC (Equality and Human Rights Commission) guidance’ in an article in TES.
The panel was asked if it felt there was a gap in the market for a ‘sensible gender service’, one which took children up to their 18th birthday without medication.
A clinician who didn’t want to take children to the clinic for medication, just treat them psychologically, said they had been told ‘we wouldn’t get any customers’. The Tavistock Trust depends on the money that comes in from that clinic. If there was a clinic that gave drugs and one that didn’t, they would all go to the one that gave the drugs.
Mention was made of the ‘two year black hole’ that families faced while waiting for an appointment after a child first ‘comes out’ as transgender and how lobby groups leap in to fill that gap with affirmation. Concerns were expressed that children were being ‘funneled into a service which is a one-way conveyor belt’.
A Director of Marketing and Communications at the Tavistock introduced herself. “It’s not a conveyor belt,’ she disagreed, advising us that the waiting list has grown, both because of the increase in referrals and also the increase in the number of appointments. She said children had between four and six assessments.
“Between three and four,” someone interrupted.
“Four to six,” she reaffirmed.
“Even twelve years ago it was three,” interjected Evans, “because I was there and I witnessed it.”
After a pause, she continued that the average number of sessions over the last five years had been seven. It takes a long time to train clinicians to do ‘incredibly difficult work’. Most of the time they worked with a dual clinician model, and “fewer than half our patients actually progress on to any kind of physical intervention of any kind”.
It was pointed out that we know younger children are less likely to receive medication, so numbers must be much higher than half for teenagers. She replied somewhat evasively that a teenager approaching the service today would be ‘unlikely to access physical intervention’. She described the situation in the US as ‘pretty dire and frightening’ but claimed the situation in the UK was different within the NHS, while expressing increasing concern about private practice and self-medication, a situation not helped by long waiting lists.
A woman asked if the panel had a comment on suicide risks. Her child had been suffering from anxiety and depression as well as gender dysphoria: she said her psychiatrist said her child had ‘a really high risk of suicide’ if she didn’t address the trans issue quickly and this caused her to seek private treatment.
“We literally don’t have the evidence to say either way, so they should not be saying that.”
Panel members agreed that the risk of suicide needed to be considered, although “a multi-analysis of European data shows the risk is hardly higher than any other group with recognisable mental disturbance”.
Acknowledging that good work went on at the Tavistock, it was observed, doesn’t address the fact that staff on Panorama and in Bells’ report are saying different things, nor that there have been five recent whistle blowers from the service.
When Marcus Evans was the clinical director for adolescent services, he told us, he had asked the medical director about outcomes in terms of how many kids go on to UCL and what happens after investigation. He was told they didn’t have the figures. This is a matter for concern.
 We need to keep dialogue open with the Tavistock, said Byng, calling it ‘probably the best service in the world’ but adding that it needs to collect proper evidence of outcomes and increase openness.
We need to keep dialogue open with the Tavistock, said Byng, calling it ‘probably the best service in the world’ but adding that it needs to collect proper evidence of outcomes and increase openness.
“Medically we need to be able to speak about this. How do we make a difference? We have conversations with everyone we meet.”
“I really have to wind things up now,” said Lord Moonie, describing the presentations as ‘covering their areas admirably’ and concluding, “I believe this is a social contagion.. if you look at society over the past hundred years there have been others and they’ve all come and they’ve all gone. … the other side know this full well… we have science and reason on our side: all they have is gender.”
It was a relief to step out of the room and into the cool air of the carpeted hallways. Interesting as the meeting had been, three hours taking frenzied notes in a small room with no coffee is no mean feat. I was more than ready to hit the pub for a pint of soda and lime. So I did.
Many thanks for this
Pingback: Another unfortunate experiment? New Zealand’s transgender health policy and its impact on childre – Redline
Pingback: Susan & Marcus Evans' 'Gender Dysphoria' - a review |Lily Maynard
Pingback: Stephanie Davies-Arai & the story of Transgender Trend -Lily Maynard