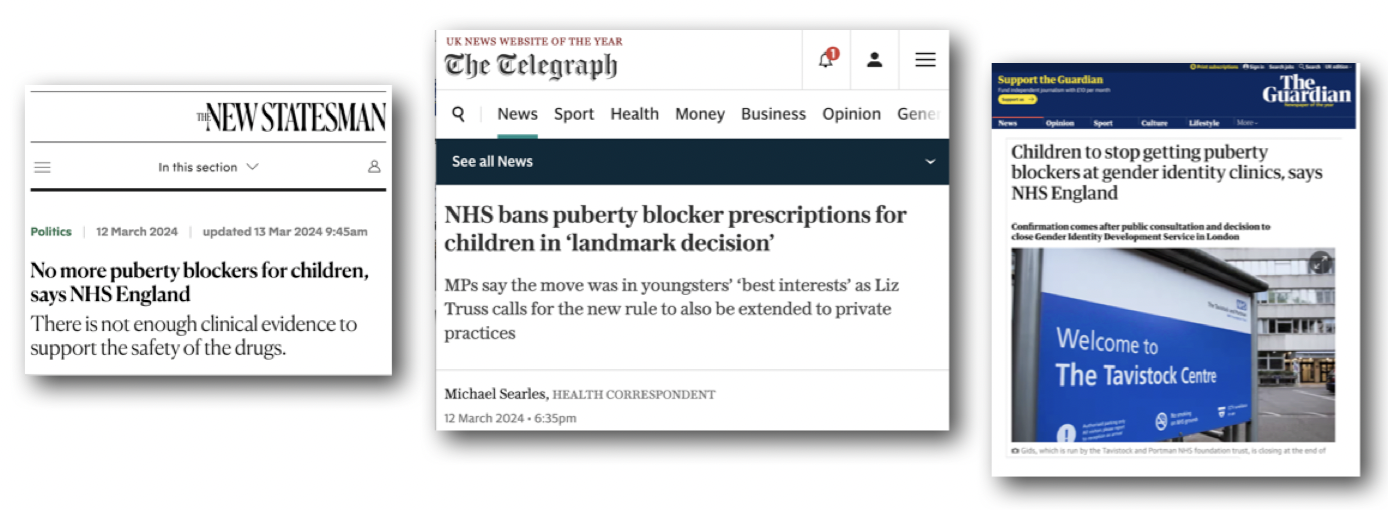
“We have concluded that there is not enough evidence to support the safety or clinical effectiveness of puberty-suppressing hormones to make the treatment routinely available at this time.”
 So announced the NHS this week (March 2024), on publication of the results of its recent consultation concerning the provision of off-label drugs to halt puberty in gender dysphoric children.
So announced the NHS this week (March 2024), on publication of the results of its recent consultation concerning the provision of off-label drugs to halt puberty in gender dysphoric children.
This is a far cry from its 2018 position that “the effects of treatment with GnRH analogues (aka ‘puberty blockers’) are considered to be fully reversible”.
This year has seen the closure of GIDS at the Tavistock (well, any day now, though it hasn’t happened yet), the promise of two new regional gender clnics, (although nobody seems sure quite when) and now confirmation of the NHS decision to ban puberty blockers. It all sounds very promising, but when you look a little closer, not a lot has changed.
Before we dive in, we should answer – what are puberty blockers and how did they start being used on gender dysphoric children?
Puberty blockers
 Michael Biggs has an excellent YouTube video which covers the basics in less than half an hour. Transgender Trend has an excellent piece here.
Michael Biggs has an excellent YouTube video which covers the basics in less than half an hour. Transgender Trend has an excellent piece here.
Puberty blockers are a class of drugs known as ‘gonadotropin-releasing hormone (GnRH) analogues’. They are produced in the hypothalamus and act on the pituitary gland to block the production of sex hormones by preventing the release of the chemical signals which stimulate the production of oestrogen and testosterone. This means the changes associated with puberty don’t happen.

AI IMAGE: puberty blockers work nothing like this
Brand names for these drugs vary, but none of them has ever been approved for use in gender dysphoric children, although they have been licenced to block precocious puberty in very young children (girls of up to age seven or boys of up to age nine).
For this reason, gender clinicians justify using them in gender dysphoric children, despite these children being a different cohort, not least in that they are older.
The Dutch Protocol
The policies followed in England, and many other countries, are based on what we call ‘The Dutch Protocol’ which was in turn based on the work of two clinicians, Louis Gooren, and Peggy Cohen-Kettenis.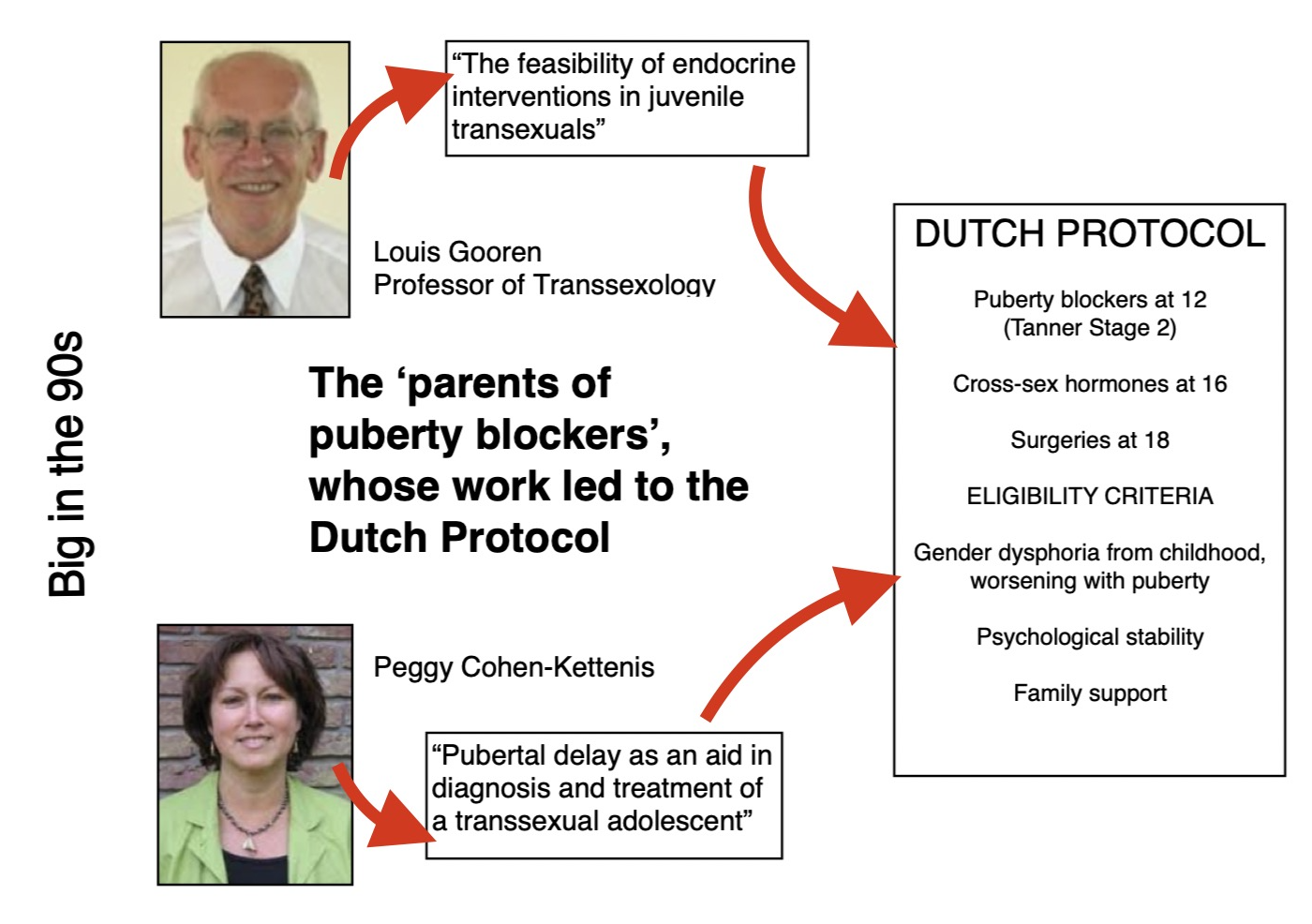
“In the Dutch protocol for the treatment of transsexual adolescents, candidates are considered eligible for the suppression of endogenous puberty when they fulfil the Diagnostic and Statistic Manual of Mental Disorders-IV-RT criteria for gender disorder, have suffered from lifelong extreme gender dysphoria, are psychologically stable and live in a supportive environment,” wrote Cohen-Kettenis and Henriëtte A Delemarre-Van de Waal in their 2006 paper Clinical Management of Gender Identity Disorder in Adolescents.
Biggs notes, in his video, that the eligibility criteria of the Dutch Protocol (gender dysphoria from childhood, increasing at puberty, psychological stability and a supportive family) is rarely adopted in England.
The article that introduced ‘puberty suppression’ to the medical community was titled ‘the feasibility of endocrine interventions in juvenile transexuals’ and it was introduced by Louis Gooren – the world’s first professor of transexology, no less!
Gooren is not to be confused with Dr Everett Scott from the Rocky Horror Picture Show, an easy mistake, I know.. 
In the introduction to the article, he (Gooren, not Scott) speaks of how many adult transexuals ‘remember puberty with abhorrence’. Gooren looked to provide the ‘magical solution’ that these transexuals retrospectively sought. Unlike Scott, who was more preoccupied with the audio-vibratory-physio-molecular transport device they possessed.
Catching them young
Clinical observations that gender dysphoria rarely resolved with psychotherapy first arose in the 80s, reported Cohen-Kettenis. “Puberty may have a strong negative impact on their (gender dysphoric children) emotional and social functioning, and even on their performance in school. Therefore, the suppression of puberty, followed by gender confirming hormonal and surgical treatment may have great benefits”.
In the Netherlands, ‘gender-affirming medical treatment’ had been available for transgender adults aged over 18 years since 1972. In 1987, Cohen-Kettenis ‘noticed an increasing number of transgender teenagers requesting medical intervention‘. So- after careful consideration, of course- the age was dropped to sixteen and GnRhAs were introduced.
The younger the child, the more malleable the clay. It figures that catching a pubescent child earlier would result in a child more likely to ‘pass’ as the opposite sex, ergo, theorises Cohen-Kettenis, a happier child.
“After the first experience with a natal girl who responded to the treatment exceptionally well, it was decided to start treatment in a large number of carefully selected adolescents.” reported Cohen-Kettenis. In addition to the criteria that had been set for the ≥16 year olds, eligible participants now had to be at least 12 years old “because it seemed to be important that adolescents experience some of the physical effects of puberty to make a well-informed decision onwhether to suppress these effects.”
Considerate indeed. Once you set off down this path, where do you stop? Allowing a child a glimpse of puberty before implicating chemical castration is being pitched as the moral choice?
Somewhere out there will be people who are mad enough to believe that Diane Ehrensaft’s ‘trans toddlers’, those hairgrip-pulling-out, onesie-unsnapping babies, should have medical interventions.
The story of B
 Cohen-Kettenis’ original study followed a single same-sex attracted patient, a gender dysphoric ‘tomboy’ called B, who was put on puberty blockers (Triptorelin) between the ages of 13-18. Treatment at a local mental health institue improved B’s depression but her ‘cross-sex behaviour, interests and identification remained’. Puberty suspension allowed her therapist to ‘explore gender issues for an extended period’ after which B fully medically transitioned between the ages of 18-20.
Cohen-Kettenis’ original study followed a single same-sex attracted patient, a gender dysphoric ‘tomboy’ called B, who was put on puberty blockers (Triptorelin) between the ages of 13-18. Treatment at a local mental health institue improved B’s depression but her ‘cross-sex behaviour, interests and identification remained’. Puberty suspension allowed her therapist to ‘explore gender issues for an extended period’ after which B fully medically transitioned between the ages of 18-20.
After blockers, testosterone, double mastectomy, hysterectomy and phalloplasty – as well as a legal sex change- B’s gender dysphoria had gone, reported Cohen-Kettenis, and she had no regrets at one year follow up.
When followed-up many years later, B, now 35, was found to be in good physical health with bone densisty ‘within the normal range for both sexes’. She still professed no regrets.
 However, B ‘had not had many steady girlfriends’ and a long-term girlfriend had recently finished things after B would not move in with her. B felt ‘he’ had pushed her away ‘due to shame about his (sic) genital appearance and his (sic) feelings of inadequacy in sexual matters’.
However, B ‘had not had many steady girlfriends’ and a long-term girlfriend had recently finished things after B would not move in with her. B felt ‘he’ had pushed her away ‘due to shame about his (sic) genital appearance and his (sic) feelings of inadequacy in sexual matters’.
B was also depressed, although not clinically so. So that’s ok.
‘Negative side effects are limited,” reported Cohen-Kettenis.
And this, dear reader, is the study on which the idea of giving children ‘time to think’ with puberty blockers is based.
What’s the problem?
It is important to be clear that both Gooren and Cohen-Kettenis were aware of the potential health problems associated with offering these drugs to children, yet they continued, and continue, to support doing so.
 “Safety considerations are to be made on short-term as well as long-term effects. Puberty is a crucial developmental phase for bone health and may also be important for cardiovascular health in adulthood…
“Safety considerations are to be made on short-term as well as long-term effects. Puberty is a crucial developmental phase for bone health and may also be important for cardiovascular health in adulthood…
…long-term follow-up studies are necessary to draw more definite conclusions. In addition to the areas that were discussed previously, there is need for MRI studies investigating the effects of GnRHa and subsequent cross-sex hormone treatment on the developing brain.”
One of the problems is that the drugs, as mentioned above, are used off label, untested for this purpose and may have both mental and physical side effects.
In 2017 it was reported in the press that many young women who had been given GnRHs (aka Lupron) when children, for precocious puberty or to increase their height, had been struck with a variety of health conditions. Some developed osteoperosis or degenerative disc diseases. One twenty-six year old needed a hip replacement. More than 10,000 adverse event  reports ‘describing everything from brittle bones to faulty joints’ have been filed with the FDA in America, reflecting the experiences of women who were given Lupron as children. Most women interviewed also reported depression or anxiety.
reports ‘describing everything from brittle bones to faulty joints’ have been filed with the FDA in America, reflecting the experiences of women who were given Lupron as children. Most women interviewed also reported depression or anxiety.
“It just feels like I’m being punished for basically being experimented on when I was a child,” said Sharissa Derricott (pictured), from Oklahoma, who has numerous health conditions. “I’d hate for a child to be put on Lupron, get to my age and go through the things I have been through.”
The same drugs are also used to treat some reproductive issues in women, such as endometriosis and uterine fibroids, and patients are advised to only take them for six months.
GnRH analogues are also used to treat some prostate or breast cancers. Side effects may include one or more of the following: Osteoporosis. Heart disease. Problems metabolising fats and sugar. Depression. Hot flashes. Anemia. Decreased libido.
Another use for GnRhs is to chemically castrate sex offenders. Side effects in one study included increased suicide ideation.
Puberty blockers have long worn the ‘harmless and reversible’ sash, but recent research is suggesting otherwise.
A 2017 study– so not so recent really, showed that sheep given ‘puberty blockers’ showed ‘a reduction in long-term spatial memory’ which ‘persists after discontinuation of peripubertal GnRH agonist treatment’.  The study concluded “GnRH irreversibly alters these cognitive functions during a critical window of development”.
The study concluded “GnRH irreversibly alters these cognitive functions during a critical window of development”.
As Alison Clayton so succinctly summarises in her 2022 paper ‘Gender-Affirming Treatment of Gender Dysphoria in Youth: A Perfect Storm Environment for the Placebo Effect’:
“If puberty blockers are commenced in early puberty and followed by cross-sex hormones, there are no proven methods of fertility preservation (Bangalore Krishna et al., 2019). Surgeries, such as gonadectomies and most genital surgeries, will result in permanent sterility. These impaired fertility and sterility outcomes are important because, firstly, as Cheng et al. (2019) reported, the widespread assumption that many transgender people do not want to have biological children is not supported by several recent studies. Secondly, children as young as ten, who do not have capacity for informed consent, are starting a treatment course that will likely render them infertile or sterile and this raises complex bioethical issues.”
(Baron & Dierckxsens, 2021).
Time to Think

‘Time to think’ is the idea that blockers provide space for a child to explore their gender identity with a therapist and as they move through the world, without the ever present Damoclesian threat of puberty hanging over their head.
The problem with the idea of blockers as a diagnostic tool is that all- with very, very few exceptions- the kids put on blockers go on to take cross-sex hormones. Rather than a pause button, it seems that puberty ‘blocking’ drugs act as a first step to transition, and the kids put on them don’t turn back. TRAs counter with the argument that this is because only the kids that are ‘really trans’ get put on blockers in the first place. And so on. Either way, puberty blockers don’t appear to provide that ‘time to think’ that they promise, nor the fix-all solution families are hoping for.
Hannah Barnes remembers GIDS being quite open about not following ‘evidence based’ practices, extending the protocols used for a specific group of dysphoric kids to treat young people with a variety of disorders. She writes about the service’s failings in her 2023 book, aptly titled, ‘Time to Think:
Reversible?
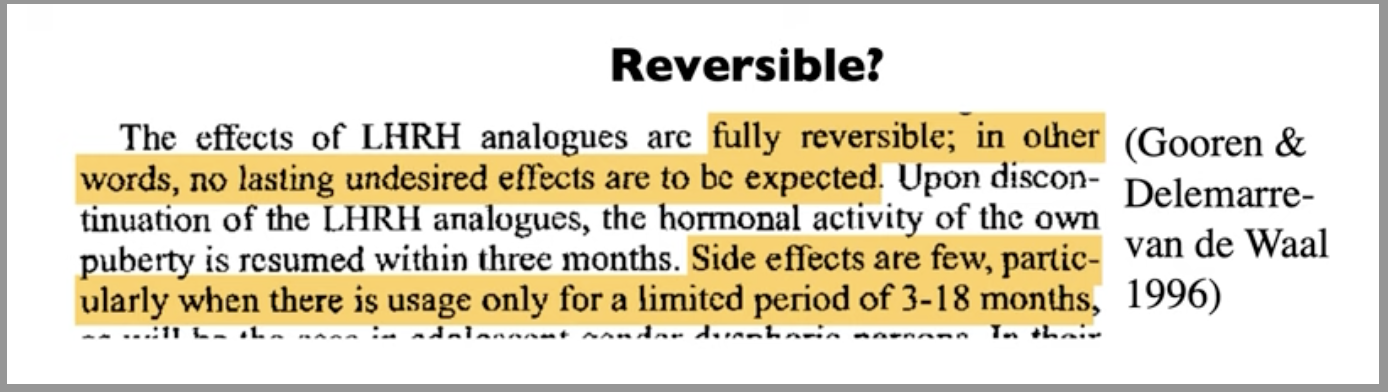 In 1996 Gooren made the claim that GnRHa ‘blockers’ were ‘fully reversible, in other words no lasting undesired effects are to be expected…. side effects are few particularly when there is usage for a limited period of 3-18 months’.
In 1996 Gooren made the claim that GnRHa ‘blockers’ were ‘fully reversible, in other words no lasting undesired effects are to be expected…. side effects are few particularly when there is usage for a limited period of 3-18 months’.
But in most cases they are not being taken for such short periods. From Cohen-Ketternis’s original study, where B spent five years on puberty blockers, to the cases of ever-younger children being prescribed them in the UK, children are not taking puberty blockers for just three months, because they are staying on them until they are allowed to move on to ‘cross-sex’ hormones.
And of course it has to be acknowledged that time does not stand still for these children. Their peer group will grow taller and wider and voices will deepen and soften, and interests and feelings will change and the puberty blocked child will have no first hand experience of these things. At puberty, the brain starts its journey into adulthood. The puberty blocked child watches from the harbour as the fleet leaves without her.
That is not reversible.
Trans the gay away
Childhood indicators of ‘trans kids’ are often said to be the toys they play with, clothes and hobbies they prefer and how boisterous or gentle they are. Well, obviously really, how else could we identify the trans child? But studies show that liking these things and identifying strongly with the toys and trimmings of the opposite sex is also an indicator for homosexuality.
Cohen-Kettenis herself noted that “several respective studies in gender atypical boys show that this childhood behaviour correlates considerably stronger with future homosexuality then with transsexualism”.
Yet at the same time she advocated for giving hormones to younger patients because “there is no reasonable expectation that their cross-sex identity will change”. So concerns were raised and circumnavigated even back then.
Biggs cites more recent data from Li Kung and Hines (2017) which showed that young boys who preferred activities usually considered to be more ‘feminine’ aged four-and a-half were far more likely to self-report as gay at age fifteen. Of course, many kids haven’t figured out their sexuality at fifteen, so the long-term figure is likely to be higher.
 In 2019, five clinicians, who had resigned from GIDS due to concerns, spoke to the Times. The paper learned that so many potentially gay children were being sent down a clinical pathway that there was a dark joke among staff that “there would be no gay people left”.
In 2019, five clinicians, who had resigned from GIDS due to concerns, spoke to the Times. The paper learned that so many potentially gay children were being sent down a clinical pathway that there was a dark joke among staff that “there would be no gay people left”.
“For some families, it was easier to say, this is a medical problem, ‘here’s my child, please fix them!’ than dealing with a young, gay kid,” a female clinician told the Times.
Remember, children put on blockers, often kids who are same-sex attracted, or autistic, or who have co-exisitng mental health issues, do not decide to stop taking them. And a child who has their puberty blocked and then goes on to take cross-sex hormones will be sterile. So now we are sterilising gay kids.
And then, after all this ‘catching them young’, the boys who have been told almost all their lives that they can be girls, and who have experienced no puberty, are left with the tiny penis of a prepubescent boy. What happens when they go on to have their penis ‘resculpted’ into an internal sheath?
 There isn’t enough tissue there to make a neo-vagina, so the process has to be padded out with a bit of gut. Yes, gut. Reality star Jazz Jennings, whose mother had a ‘bye bye penis’ cake baked for him, was one such patient. His neo-vagina ‘split’ with an audible ‘pop’ and had to be reconstructed.
There isn’t enough tissue there to make a neo-vagina, so the process has to be padded out with a bit of gut. Yes, gut. Reality star Jazz Jennings, whose mother had a ‘bye bye penis’ cake baked for him, was one such patient. His neo-vagina ‘split’ with an audible ‘pop’ and had to be reconstructed.
So there’s that to consider.
GIDS and puberty blockers at the Tavistock
“The Tavistock GIDS began an ‘Early Intervention study’ in 2011. Previous to this, puberty blockers were offered as a treatment only to children from the age of sixteen. The trial lowered the age to twelve, and subsequently, by 2014, to any child who had reached Tanner Stage 2 of puberty. This meant that now children as young as ten could be given blockers. To date GIDS has treated over a thousand children with puberty blockers, with about 230 of these children under the age of 14, the youngest child being 10 years old. – Transgender Trend
Concerns about GIDS referrals for puberty blockers were first raised by whistleblower Sue Evans back in 2005. Since then the referrals increased and the children got younger, until by 2016 hundreds of children were taking them. It is estimated that currently around 100 GIDS patients are receiving puberty blockers.
As I write, despite all the hooha, GIDS at the Tavistock has not even closed.
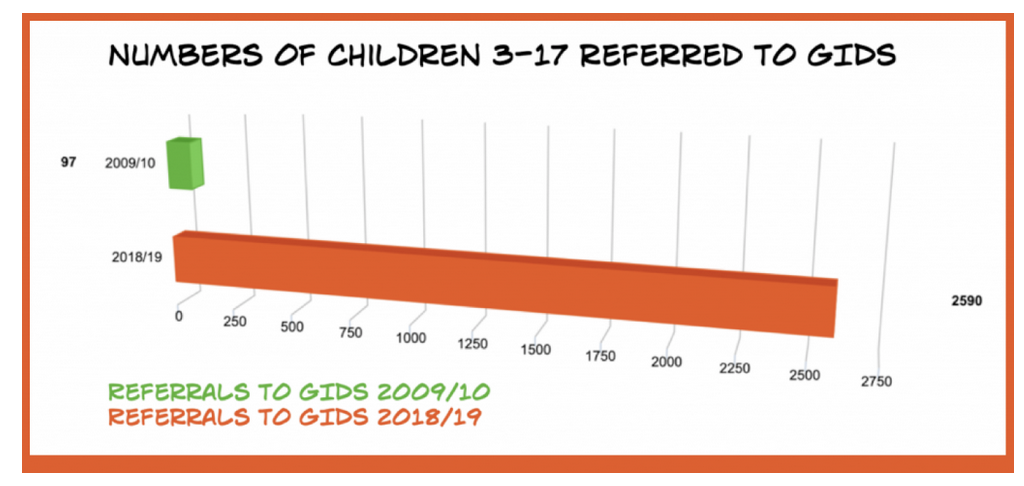 You may be aware of the huge increase of referrals of children seeking service from the GIDS (Gender Identity Development Service) between 2009/10 and 2018/19, and the spotlight this threw on the ever-popular use of puberty blockers.
You may be aware of the huge increase of referrals of children seeking service from the GIDS (Gender Identity Development Service) between 2009/10 and 2018/19, and the spotlight this threw on the ever-popular use of puberty blockers.
In 2019, five clinicians whjo had resigned from GIDS due to concerns spoke to the Times, which reported: “There used to be about 50 referrals (to GIDS) a year, mainly males with a history of gender issues. Now there are thousands of young females reporting a sudden gender crisis for the first time.”
“If someone was suggesting plastic surgery or any other permanent change we’d be saying, hang on a minute.” observed one ex-clnician.
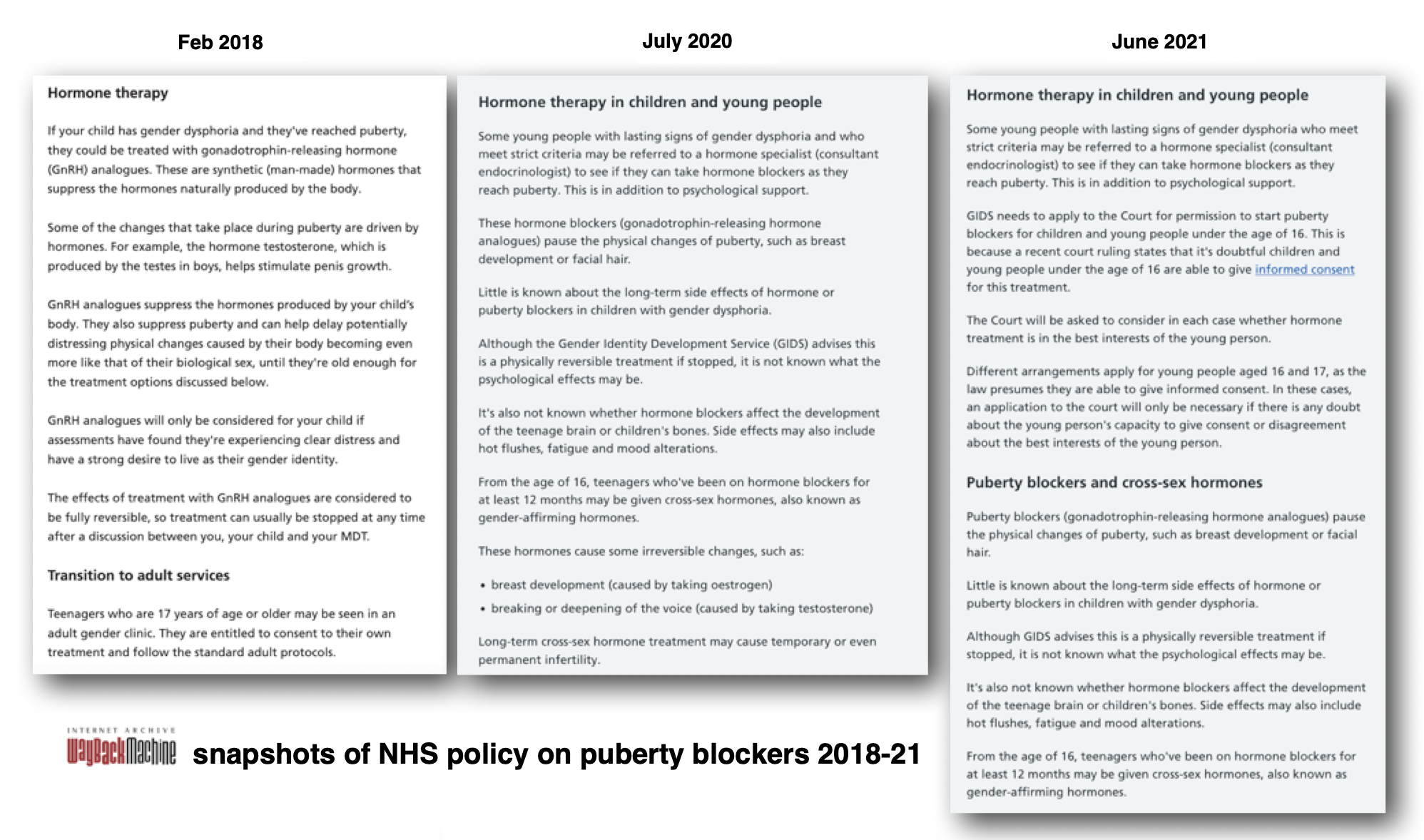
I visited Wayback Machine to collect snapshots of the ever-changing NHS policy on giving blockers and cross-sex hormones to children. Snapshots from the NHS page on gender dysphoria from Feb 2018, July 2020 and June 2021 are below.
The 2018 guidance was changed after the first Kiera Bell case in 2020 and again when the case was overruled in 2021. You can see that there are differences in the age at which children are referred to adult services (it drops from 17 to 16) and how the guidance changes alongside judgement from the courts.
2018
In 2018, the NHS was asserting “the effects of treatment with GnRH analogues (aka ‘puberty blockers) are considered to be fully reversible”.
2020
The 2018 advice was changed in June 2020 from ‘your child’ to ‘some young people with lasting signs of gender dysphoria and who meet strict criteria’. Among other things, references to penis growth were removed and the age of referral to adult services was dropped from 17 to 16.
In 2020 a judicial review was brought by former Tavistock psychiatrist Susan Evans against the Tavistock & Portman NHS Trust. Claimants Keira Bell and Mrs A against the Tavistock (2021) and the work done both up front and behind the scenes by organisations like Transgender Trend, and the public eye became very much fixed upon the issue.
In the 2020 ‘Kiera Bell Case’, the High Court ruled that patients under sixteen were unlikely to be able to fully understand the criteria required for them to give informed consent to puberty-blocking drugs.
At the time, GIDS had a waiting list of 5,000 children, was seeing 3,000 children and prescribing blockers or cross sex hormones for several hundred of those.
The 2020 ruling declared that children could not be prescribed these medical interventions without permission from a court. 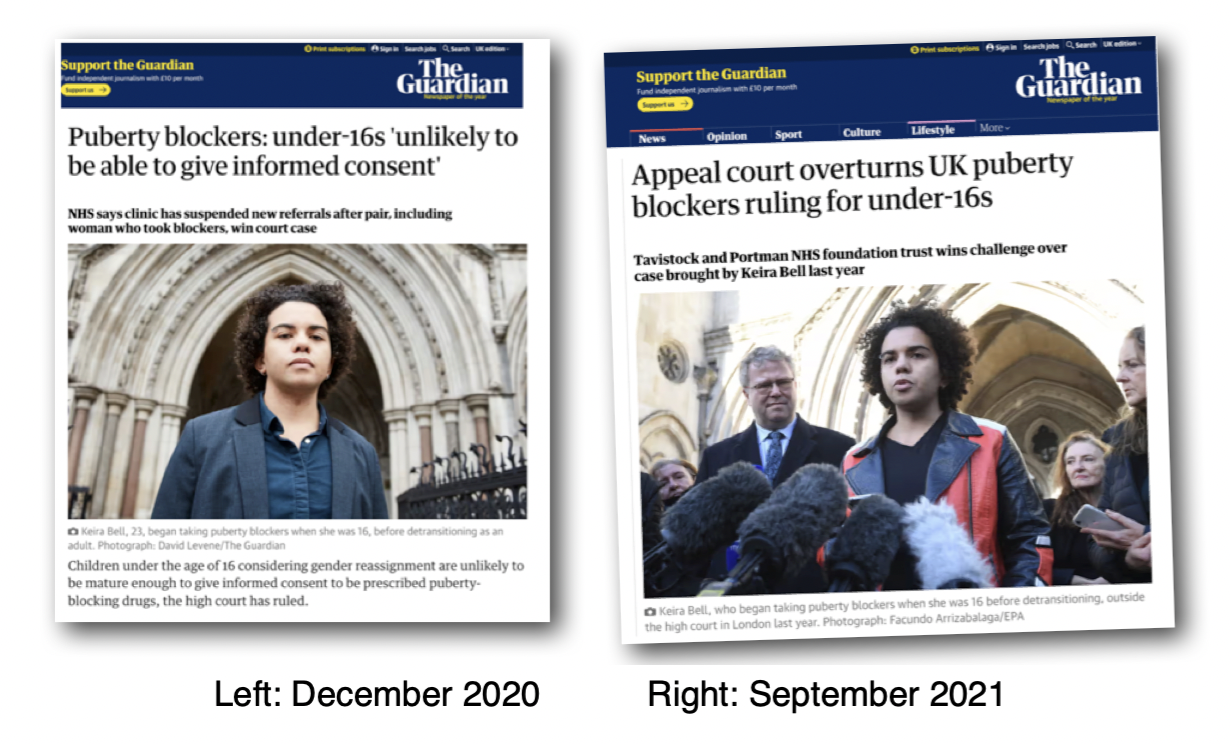
Barely was the ink dry on the ruling than the decision was overturned in September 2021. Appeal court judges stressed that it was established legal principle for “clinicians rather than the court to decide on competence (ability to consent)”.
In July 2020 (see above) the NHS webpage was amended again.
“Little is known about the long-term side-effects of hormones or puberty blockers in children with gender dysphoria. Although GIDS advises this is a physically reversible treatment if stopped, it is not known what the psychological effects may be.
It is not known whether hormone blockers affect the development of the teenage brain or children’s bones. Side effects may also include hot flushes, fatigue and mood alterations”.
In 2021 the same warnings were present on the NHS website, until June, after the court ruling, when the page was changed: “GIDS needs to apply to the court for permission to start puberty blockers… a recent court ruling states that it is doubtful that children and young people under the age of sixteen are able to give informed consent”.
The page carried a lengthier warning as to potential side effects and this stayed in place for just five months, until the middle of November 2021 when it was changed again.
In November 2021 the judgement was overruled and the NHS removed the reference to applying to the court.
This all resulted in the Cass Review. Dr Hilary Cass published her interim report in February 2022, which set out her initial findings and advice from her review. Cass noted that some NHS staff reported feeling “under pressure to adopt an unquestioning affirmative approach and that this is at odds with the standard process of clinical assessment and diagnosis that they have been trained to undertake in all other clinical encounters.”
Inspectors rated the service ‘inadequate’ and this all resulted, ultimately, in the July 2022 announcement that GIDS would close. NHS England confirmed that young people who were already receiving blockers would continue to do so.
 In November 2023 the Telegraph reported that despite the previous summer’s announcement, the number of children prescribed puberty blockers had doubled since the National Health Service promised to curb the practice.
In November 2023 the Telegraph reported that despite the previous summer’s announcement, the number of children prescribed puberty blockers had doubled since the National Health Service promised to curb the practice.
“At least 100 children – some as young as 12 – have been put on the drugs to prevent puberty since July 2022, when health officials said the practice would be stopped outside of clinical trials after a damning review of children’s gender services.”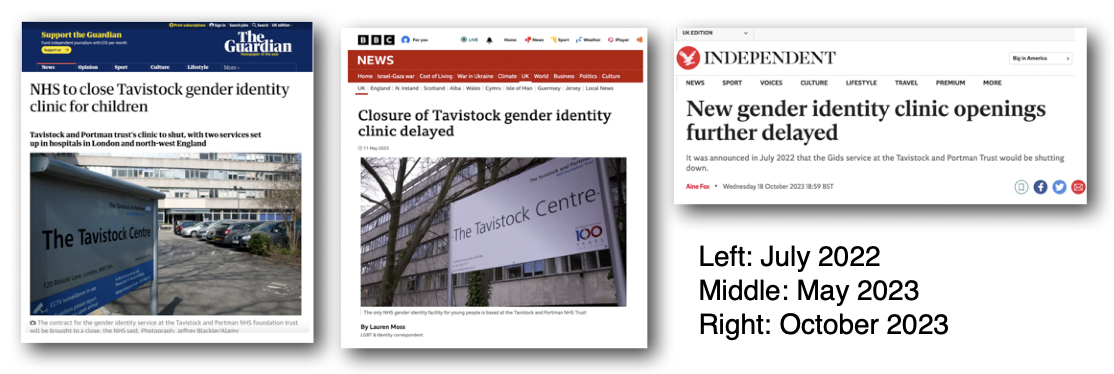
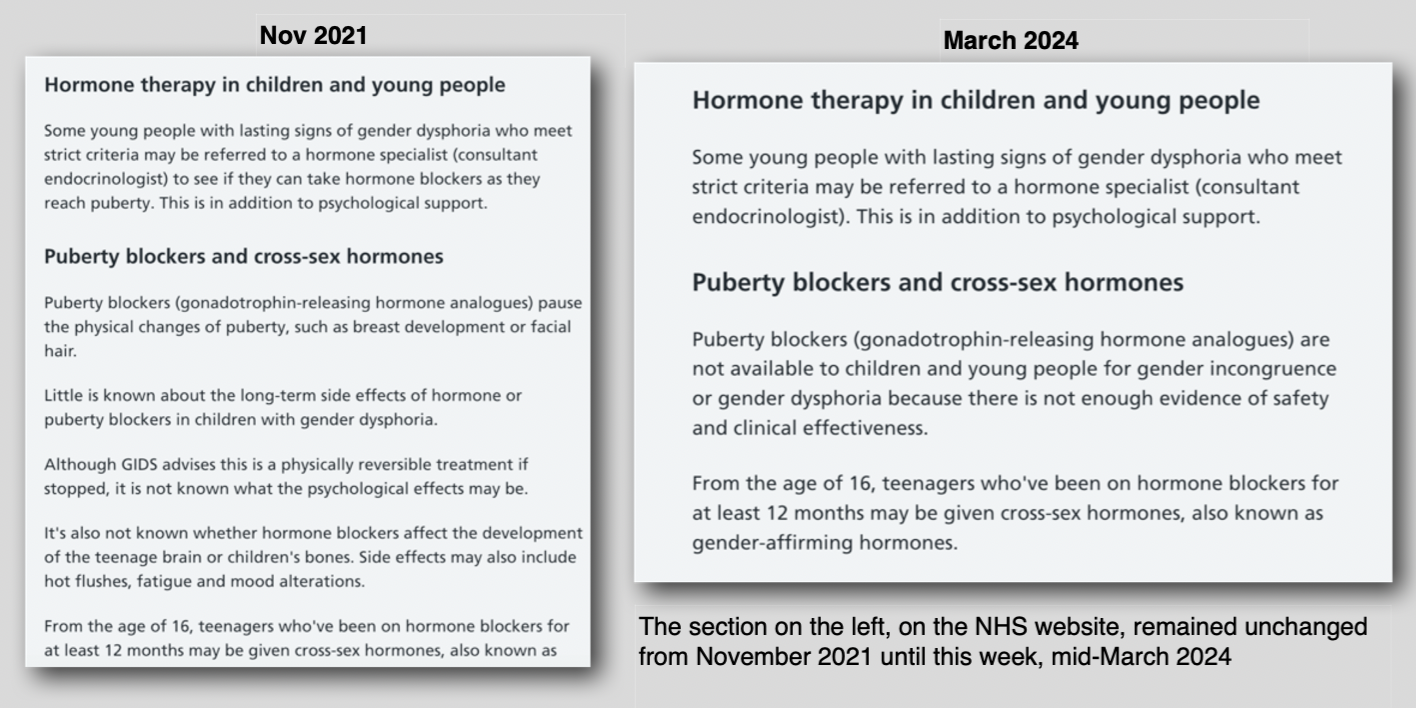
The November 2021 guidance remained in place on the NHS website until it was amended on 13th March 2024.
In June 2023 the NHS announced that following “advice from Dr Hilary Cass’ Independent Review highlighting the significant uncertainties surrounding the use of hormone treatments” they wished to make clear “that the NHS will only commission puberty supressing hormones as part of clinical research.”
They then went on to use an awful lot of words to say, basically, that there was going to be ‘A Study’. It would be overseen by a new national Children and Young People’s Gender Dysphoria Research Oversight Board and it would look into the impact of puberty suppressing hormones (‘puberty blockers’) on gender dysphoria in children and young people with early-onset gender dysphoria.
The Consultation
You can see the current NHS page on Gender Dysphoria here. The NHS consultation (now closed) ran for 90 days from 3 August to 1 November 2023. The public consultation guide can be viewed here.
 An analysis of the results of the consultation can be viewed here. It was highly politicised with groups on both sides offering advice to the public on how to complete the forms, and TRA organisations including Stonewall and Mermaids framing it as ‘a dangerous roll back of healthcare for trans children’.
An analysis of the results of the consultation can be viewed here. It was highly politicised with groups on both sides offering advice to the public on how to complete the forms, and TRA organisations including Stonewall and Mermaids framing it as ‘a dangerous roll back of healthcare for trans children’. 
For an intelligent, informed take, you can read Transgender Trend’s response to the consultation here. Transgender Trend has been expressing concerns about the medicalisation of gender dysphoric children since 2016. For further information on puberty blockers you could start here.
“We welcome the proposal to stop the routine prescription of puberty suppressing hormones to children with gender-related distress and to offer psychological approaches as an alternative.” Transgender Trend
A total of 4,040 responses to the consultation were received. The report states that “broadly speaking, responses to the three open-ended questions corresponded with one of two viewpoints”. 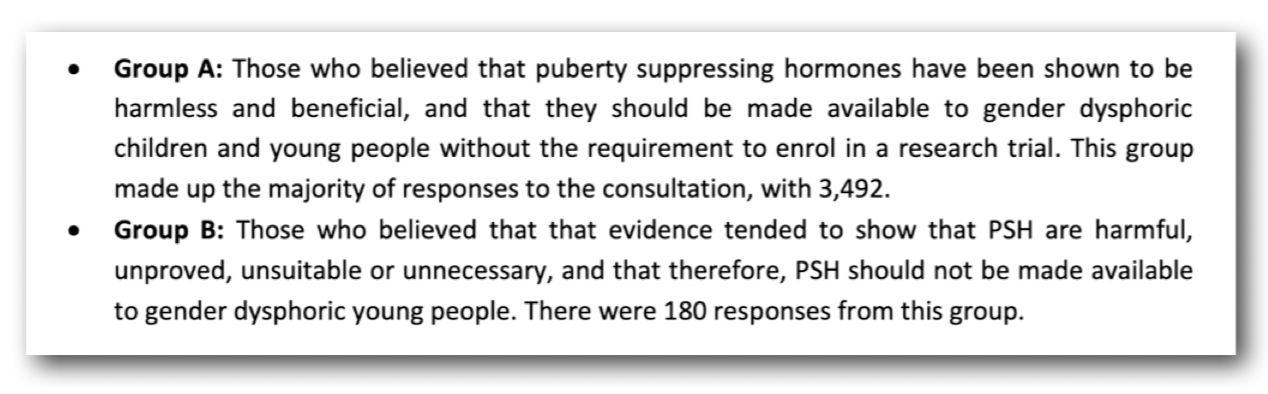
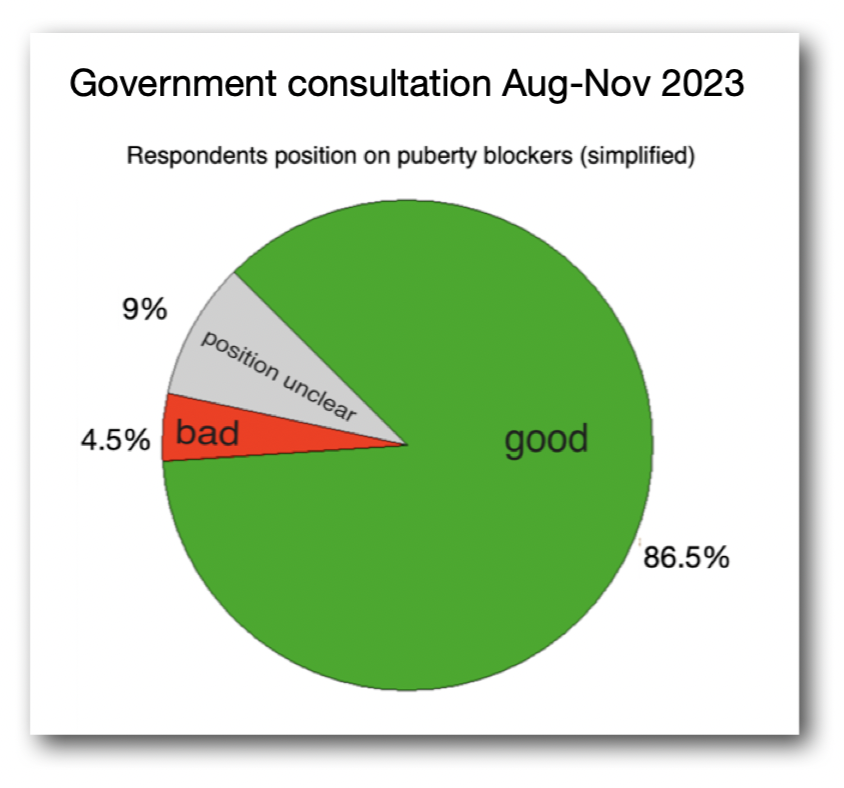 I was surprised to find that more than four out of five respondents were cheerleading for the continued use of puberty blockers. Graph on left is my own.
I was surprised to find that more than four out of five respondents were cheerleading for the continued use of puberty blockers. Graph on left is my own.
>86% of respondents to the consultation believed that blockers were harmless and should be made available to children.
Just <5% of respondents believed that blockers were harmful and should not be made available to children.
<10% did not make their position clear.
Yes, you got it, a whopping 86% of respondents reckoned that stopping a confused child from going through puberty is a good idea.
“Bring on the blockers please – we’re British!”
No
The NHS response, while not a surprise to those of us with our ears to the ground, flew in the face of the consultation results and was not met with joy from all sides.
Mermaids called the announcement ‘deeply disappointing’ and accused the NHS of “failing trans youth’.
Pink News called it ‘a new blow to gender-affirming healthcare’, seeming to forget that it- and a dozen more august periodicals- had reported on the very same thing as long ago as last June when the government announced its interim policy.
“…outside of a research setting, puberty-suppressing hormones should not be routinely commissioned for children and adolescents.”
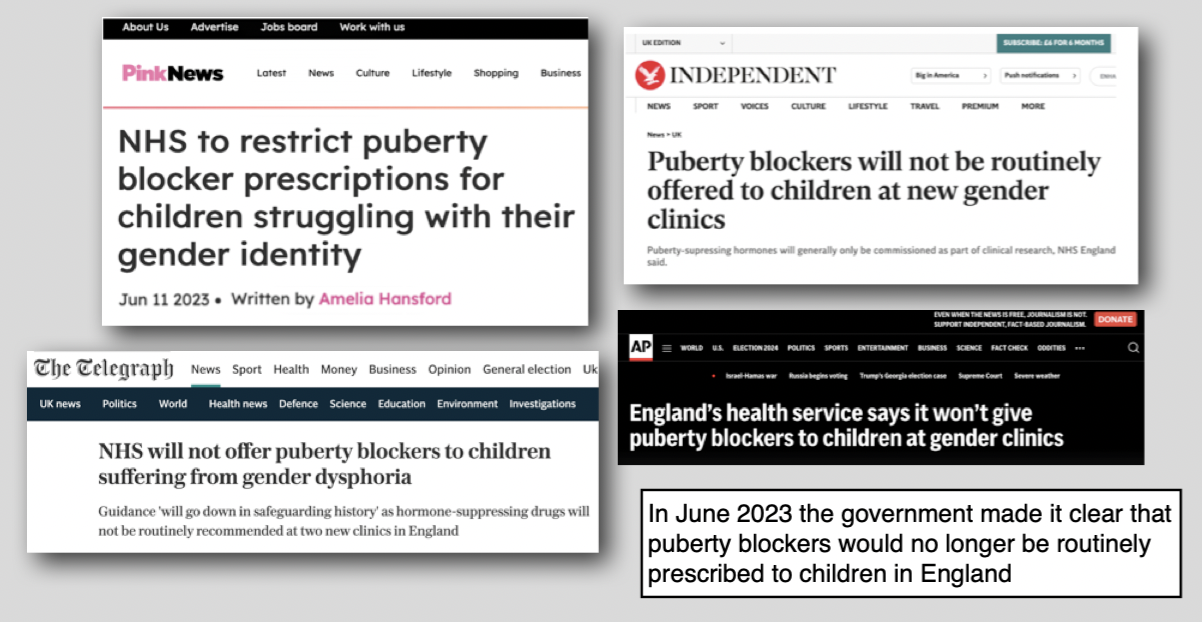
The Telegraph, back in June 2023, reported that the guidance would ‘go down in safeguarding history’ and quoted James Esses: “This will hopefully bring an end to vulnerable children being placed down a pathway to irreversible harm,” and David Bell: “All the evidence shows that puberty blockers don’t help, and there is clear evidence of physical and psychological harm caused by them.”
So many of us were a little bemused by the excitement generated by this week’s announcement.
On 12th March 2024 the NHS officially released the new clinical policy on ‘puberty suppressing hormones’ (PSH) for children and young people who have gender incongruence/gender dysphoria.
And while it’s not really new-news, it is good news. Not that good though. Don’t break out the party cups just yet.
Now it has been officially announced, and the NHS website amended, it would be easy to think there will be no more puberty blockers. But there are caveats.
Exceptional Circumstances
 “A spokesman confirmed that children treated at the new gender clinics would not be routinely offered puberty blockers as part of their treatment, but there may be exceptional circumstances in which a clinician could make a case for a child to have them.”
“A spokesman confirmed that children treated at the new gender clinics would not be routinely offered puberty blockers as part of their treatment, but there may be exceptional circumstances in which a clinician could make a case for a child to have them.”

Daily Telegraph June 2023.
How different are 2024’s ‘exceptional circumstances’ from 2020’s ‘strict criteria’?
As Transgender Trend observed in 2021, one in every seven medical referrals to GIDS between 2009-2019 medically transitioned. Is one child in seven ‘exceptional circumstances’?
However, since that announcement last summer, the government has announced that there will be no exceptional circumstances. Instead, a child’s clinician would have to apply under an NHSE ‘Individual Funding Request’ process. They would need to explain why ‘a treatment that is not routinely commissioned by the NHS is an appropriate treatment option’. Such a path is unlikely to get approval. But who knows?
Clinical Trials
“NHS England hopes to have a study into their use in place by December,” reported Sky News, “With the eligibility criteria yet to be decided.”
 A study. I hear this news with trepidation. Some of you may have read my piece Costing the Kool-Aid. In 2020 I saw leaked documents and wrote about the mostly-wacky research team whose work eventually led to the ‘HealthTalk’ page on puberty blockers.
A study. I hear this news with trepidation. Some of you may have read my piece Costing the Kool-Aid. In 2020 I saw leaked documents and wrote about the mostly-wacky research team whose work eventually led to the ‘HealthTalk’ page on puberty blockers.
At the time I wrote: “If everyone involved in recruiting young people for the project believes there should be less gatekeeping and easier access to hormones and surgeries for young people, then that is exactly what the researchers are going to find is needed.”
 And, lo and behold, fast forward and we see that was exacty what they did find was needed!
And, lo and behold, fast forward and we see that was exacty what they did find was needed!
On the ‘HealthTalk’ page we hear the tale of a mother who wants blockers for her pre-pubescent daughter because “Im really hopeful that hes (sic) gonna get the blockers in time, to not make him need top surgery… hes (sic) gonna feel really, really down if hes (sic) made to experience having breasts, basically.”
Another mum “supported her son (sic) starting hormone blockers to put his(sic) worries about unwanted puberty changes on the back burner” .
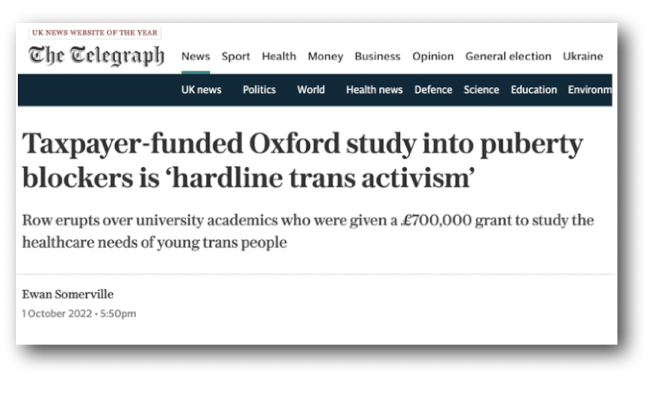 One parent told the Telegraph:
One parent told the Telegraph:
“Trans rights activists have hijacked this study, they’ve used it as a figleaf for hardline trans activism and have recruited from a very narrow selection of channels.
…the whole purpose of the study was to push for barrierless medication for children as quickly as possible, that was the starting point. It is textbook institutional capture.”
Here is the Kool-Aid Crew’s view on lovely, harmless, reversible puberty blockers:
 “Hormone blockers, also called puberty blockers, pause the physical changes of puberty that can be distressing for many trans or gender diverse young people… According to the GIDS, 2020, hormone blockers are a reversible intervention, and the WPATH cite hormone blockers in their established internationally accepted Standards of Care (SOC) guidance. This guidance states that it is more harmful to withhold this intervention that to provide it.”
“Hormone blockers, also called puberty blockers, pause the physical changes of puberty that can be distressing for many trans or gender diverse young people… According to the GIDS, 2020, hormone blockers are a reversible intervention, and the WPATH cite hormone blockers in their established internationally accepted Standards of Care (SOC) guidance. This guidance states that it is more harmful to withhold this intervention that to provide it.”
This page is still on the HealthTalk website (archived here) as of 17/3/24. Perhaps they might want to think about amending or removing it.
But they probably won’t.
The New Order of Puberty Blockers
I know nothing about the team who will head this new NHS study. Obviously it will be very different to the one cited above. I hope the team are objective, and cautious. In a climate so politically dangerous, and looking at those who control the current narrative, it is hard to see how that could be possible.
So most of all I hope that it is decided that that clinical trials are unethical and should not progress. These are experiments on children, no more, no less. Some TRAs are also unhappy about the idea of trials, viewing them as forced compliance into receiving medical care.
Where would the kids for these clinicial trials come from? The same cohort that would have been seen at the Tavistock had it remained open.
It has been confirmed that the <100 children currently receiving blockers on the NHS will continue to receive them.
And the new smaller hubs that are supposedly going to spring up around the country- if they ever get started- will surely have reason to enlist ‘trans kids’ in the great puberty blockers experiment. After all, this is groundbreaking research and a lot of people have a vested interest in the results.
As Transgender Trend observed in 2021:
“There have been a total of 5358 childhood referrals to GIDS since they opened in 2009. 800 of these 5358 have gone on to take puberty blockers. Once on puberty blockers virtually all go on to sex hormones. So that’s one in every seven referrals medically transitioning.”
It suggests that there will be plenty of takers for these medical trials.
As GIDS closes its doors at the end of this month (March 2024) you might be tempted to think the whole puberty blockers fiasco was coming to an end. I mean, at least UK kids can’t get blockers outside of the exceptional circumstances and the medical trials. Right? Right?
The Sandyford
 The SNP has refused to ban puberty blockers on the NHS in Scotland, despite this week’s announcement.
The SNP has refused to ban puberty blockers on the NHS in Scotland, despite this week’s announcement.
After a Daily Mail report in 2022, that the Sandyford Clinic in Glasgow was prescribing blockers to children as young as nine, there were calls for the clinic to be closed. This has not happened.
The Sandyford Clinic, reported the Telegraph this week, will “continue to refer children to endocrinologists for possible prescription of puberty blockers, despite an independent NHS England review warning their use could not be justified due to safety concerns.”

In the same article, the Telegrah observed that latest WPATH guidelines “support puberty-blocking hormones… and endorse permanent gender reassignment surgery for adolescents.”
The Private Sector
We know that there’s a private sector catering to the over sixteens market, everybody’s favourite uncle Stuart Lorimer has been doing that for ages (see my 2019 piece ‘Dr Lorimer brings all the ‘transboys’ to the yard’). But there’s always room for another player in a growing market.
 Some of the clinicians who have left GIDS have started up their own private ‘healthcare’ businesses.
Some of the clinicians who have left GIDS have started up their own private ‘healthcare’ businesses.
Neophyte ‘Gender Plus’ already has offices in London, Dublin and Birmingham; a new, private clinic that offers private treatments to children aged sixteen and over who have been assessed for six sessions.
Approved by England’s Care Quality Commission, the announcement was heralded by the British press just two months before confirmation of the new NHS position on blockers.
“Our team are experts in the field (many have worked for several years in NHS gender services) and feel passionately about the rights of the transgender and non-binary population to access appropriate care,” say Gender Plus.
Which, if the pictures on their website (below) are anything to go by, may or may not involve snorting lines of rainbow coloured hormones off a unicorn’s back.
The ‘team’ all have their pronouns in their bios – of course they do- and are a veritable smorgasbord of psychologists and psychotherapists. There’s also one actual psychiatrist who, unlike the others, remains faceless and who ‘completed a psychiatric training in Oxford’ (in Oxford not at Oxford, note). Oh and there’s an ex-Tavi service administrator with an anime character for a profile pic.
Unsurprisingly, Gender Plus finds NHS England’s decision to stop prescribing puberty blockers to children ‘deeply troubling‘ and believes it ‘lacks clear rationale‘.
The Gender Plus blog features a waffly piece about a ban on conversion therapy being needed because ‘trans peole have always existed’, gender identity is ‘something as innate as eye colour’ and a ban would validate the trans identities of those who had gone before.
Conversion therapy is, in case you have forgotten, that heinous practice of telling a girl she is a girl, or a boy he is a boy, and trying to explore what might make them feel they were the opposite sex. Never fear. At Gender Plus you can be assured that a highly paid trained team of therapists will affirm your delusions at every turn.
With Churchillian zeal, Gender Plus asserts, ‘this decision by NHSE will not deter this small group of young people from accessing hormone blockers, instead it will push patients and their parents down unofficial routes’.
Routes which currently do not lead to GenderPlus’s bank accounts. Boo hoo.
GenderPlus does not deal with kids under sixteen, so that’s something.
But wait! Who is this?
“Our vision is to provide low-cost, timely, accessible private healthcare – for everyone – wherever they are, whoever they are and however old they are.”
Gender GP
Like Weebles that wobble but won’t fall down, hubby & wifey duo Helen and Mike Webberley are currently up again, and running a bigger and broader Gender GP (GGP) clinic than ever before.

Shut down in the UK, they now run a Worldwide Transgender Clinic offering Health and Wellbeing Services. Here you can ‘start or continue your transition’. GGP wants ‘to put you in charge of your gender journey’ and is quick to remind you that it is possible to switch between private and public healthcare.
“At GenderGP we are always looking for ways to help make private healthcare more affordable and accessible, while you wait for public health services.”
How young is too young? I couldn’t find anything on their website beyond the bold and zealous claim that they want to provide healthcare for people ‘however old they are’.
A trip to Reddit threw up a post ostensibly from a woman wanting to get hormones for her child from GenderGP. The post received, among others, this response claiming that getting blockers for 12 year olds from GGP is ‘plain sailing’ and that ‘they’ll practically throw them at you.” GGP observes that sadly ‘it’s a bit of a postcode lottery’ as to how helpful GPs are. But they remind potential clients that “patients who have had a private consultation for investigations and diagnosis may transfer to the NHS for any subsequent treatment.”
GGP observes that sadly ‘it’s a bit of a postcode lottery’ as to how helpful GPs are. But they remind potential clients that “patients who have had a private consultation for investigations and diagnosis may transfer to the NHS for any subsequent treatment.”
Another GGP user on the Reddit thread above explains how they did just that- got one private prescription of hormones from GGP before transfering onto the NHS via their own doctor.
A third young woman relates how she contacted GGP ‘in March’ and a few weeks later received an email containing her first prescription of testosterone. Her estrogen levels are ‘a bit higher than they should be’ but it’s ok because she can ‘tell the gel is working’.

But I digress. Hapless young women who have reached the age of majority are not the concern of this piece. Nor even are the thirteen year olds on testosterone. We are, after all, here to focus on puberty blockers, not the cross-sex hormones that invariably follow them.
Follow the Money
 Jennifer Bilek writes about the billionaires who ‘fund the transgender lobby and organizations through their own organizations, including corporations’, in her piece ‘Who Are the Rich, White Men Institutionalizing Transgender Ideology?’
Jennifer Bilek writes about the billionaires who ‘fund the transgender lobby and organizations through their own organizations, including corporations’, in her piece ‘Who Are the Rich, White Men Institutionalizing Transgender Ideology?’
It’s quite a read.
Between 2003 and 2013, she reports, funding for transgender issues in the USA increased more than eightfold reaching a record high of $8.3 million. The same source that gave Bilek her figures tells us that in the following five years it more than tripled, reaching a high of $28.6 million in 2018. The 2024 figure? You tell me.
Social media is now home to a score of wealthy, fashionable, ghoulsih influencer ‘gender surgeons’ such as Sidbh Gallagher and Giancarlo McEvenue and their thousands of teenage fans.
 Here in the UK, a pharmaceutical firm that markets GnRH analogues gave a cool £100,000 to the Liberal Democrats in 2019.
Here in the UK, a pharmaceutical firm that markets GnRH analogues gave a cool £100,000 to the Liberal Democrats in 2019.
I am just touching the tip of the iceberg here.
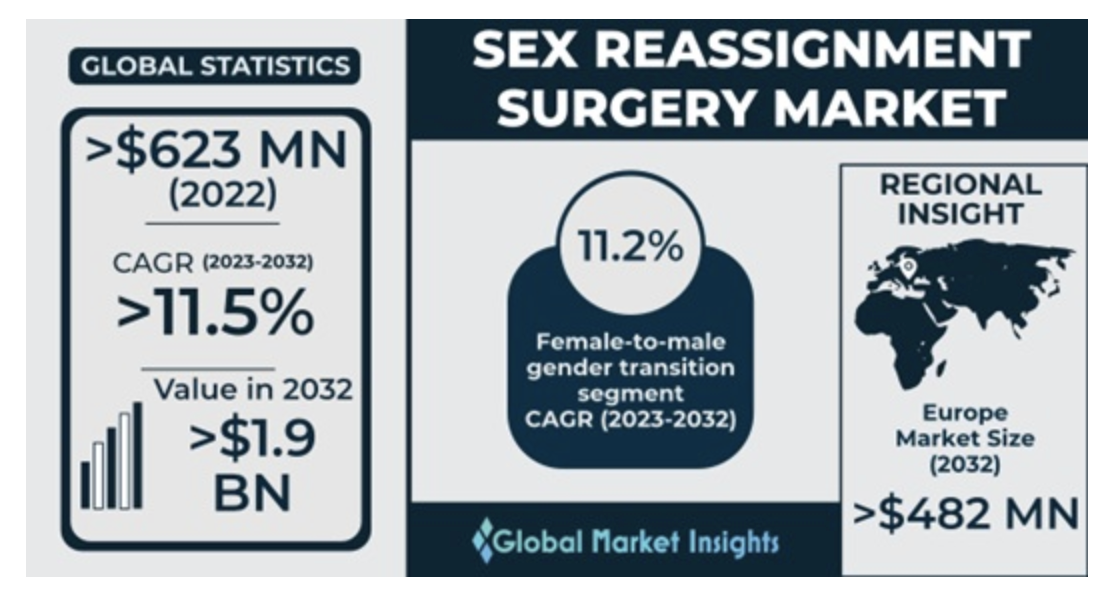 Global Market Insights set the global sex reassignment market at upwards of $63 million (around £50,000,000) and rising.
Global Market Insights set the global sex reassignment market at upwards of $63 million (around £50,000,000) and rising.
“High costs associated with sex reassignment procedures may hamper the sex reassignment surgery market revenue female to male gender change surgeries such as hysterectomy and phalloplasty are mostly expensive and not affordable by all for example the average cost of female to male sex reassignment surgery in Europe costs around 12,000 to 20,000 U.S. dollars and is anticipated to increase in the coming years.”
So let’s not dismiss those who say the trans agenda is- at least in part- driven by money. There’s a lot to be made.
 I peruse the GGP website. I learn that ‘Discovery Sessions’ are optional but ‘Information Gathering Sessions’ are compulsory. Self-reflection is less important than getting the paperwork right.
I peruse the GGP website. I learn that ‘Discovery Sessions’ are optional but ‘Information Gathering Sessions’ are compulsory. Self-reflection is less important than getting the paperwork right.
Puberty blocking injections cost from £270 for a three month supply and puberty blocking nasal spray costs £70-£90 for a one month supply. There’s also a £195 sign up fee and a subscription service of £30 a month. Plus blood tests and a yearly physical.
So pricey, yes, the basics look to come in at around >£2,000 a year for puberty blockers. But many parents spend that much on theatre classes and dance costumes.
 Gender Plus charges £275 for a one hour appointment, and at least six appointments are needed for 16-18 year olds. Non-assessment psychological support and famnily sessions are a snip at £150 per 50 mins. Gender Plus’s booking system automatically generates a zoom meeting, but in-person appointments are available. Only one in-person appointment for under 18s is usually necessary, so that’s convenient. They are ‘happy to consider a transfer from other providers’.
Gender Plus charges £275 for a one hour appointment, and at least six appointments are needed for 16-18 year olds. Non-assessment psychological support and famnily sessions are a snip at £150 per 50 mins. Gender Plus’s booking system automatically generates a zoom meeting, but in-person appointments are available. Only one in-person appointment for under 18s is usually necessary, so that’s convenient. They are ‘happy to consider a transfer from other providers’.
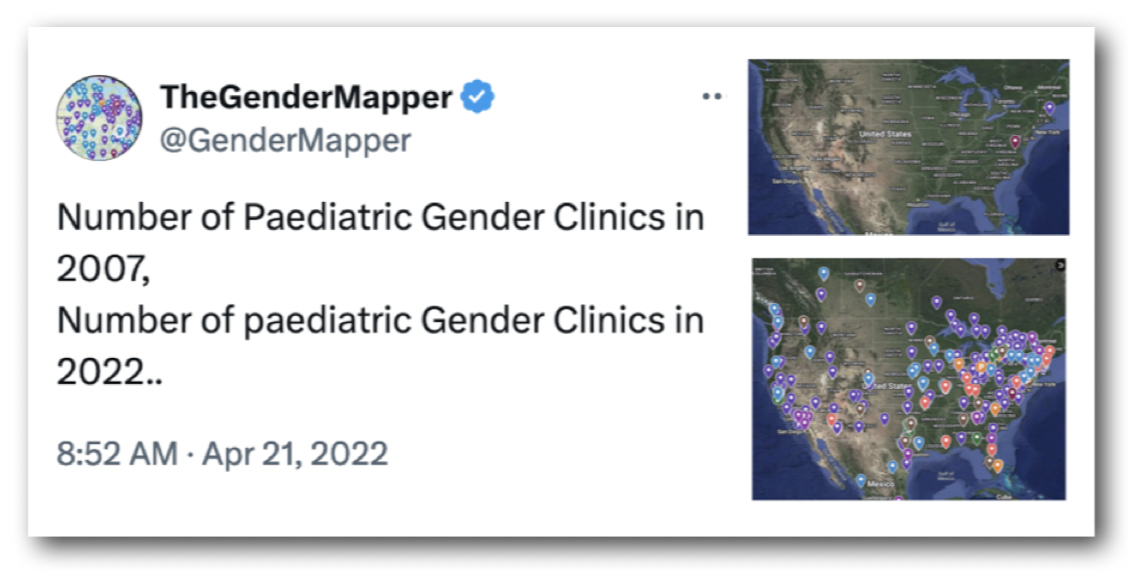
The first gender clinic for children opened in Boston in 2007. Gender Mapper follows and charts the growth of these clinics and released the maps below. That is in America, of course, and obviously it could never happen here.
Why might a parent let their child go on blockers?
Some parents will be happy to pay for medication or desperate to get their child onto these trials. They may have strict gendered expectations of their offspring, or religious reservations about a gay child. One parent was overheard at a GIDS family day saying they didn’t want their child having any gay friends because of the ‘hedonistic lifestyle’.
Some parents are just certain their kid is super-special. We’ve all met That Parent. What else could possibly induce a parent to label their offspring ‘non-binary’? It’s utter madness. Some of you may remember the ‘indigo kids’ so popular around the turn of the century. There are parents who think their kids can only be special if other people’s aren’t. But I don’t think most parents of trans kids fall into that category.
 Some parents may have reservations, but worry that their child will be at risk of suicide if not started down a medical pathway. There are plenty of organisations and individuals around shouting that ‘trans kids’ deprived of blockers are at risk of suicide.
Some parents may have reservations, but worry that their child will be at risk of suicide if not started down a medical pathway. There are plenty of organisations and individuals around shouting that ‘trans kids’ deprived of blockers are at risk of suicide.
The ‘do you want a live daughter or a dead son?’ line still hangs heavy in the air although it is dragged out less often since data emerged showing that trans-identified children were at no more risk than any other child under CAMHS. That is not to belittle that risk. And it’s hard to drown those voices out.
Some kids are groomed online to threaten suicide to get what they want. Some kids have been told they won’t be taken seriously unless they threaten suicide. There are plenty of trans-identified men (usually with 18+ accounts) who will ‘help’ a child access cheap blockers. Children may be buying pills from strangers online, or threaten to do so.
Other kids may genuinely be suicidal. Every parent’s worst nightmare. A desperate parent takes a gamble… and here come the nice men and women in white coats to make it all ok.
 A child may have co-existing conditions or issues, parents may have been told that resolving the gender issue will fix everything. Oh, what a promise! Most parents want everything to be ok for their kids, more than anything. And it might work.
A child may have co-existing conditions or issues, parents may have been told that resolving the gender issue will fix everything. Oh, what a promise! Most parents want everything to be ok for their kids, more than anything. And it might work.
Their kids’ school may well be a Stonewall Champion. Our local secondary has an LGBTQ+ club run by two ‘non-binary’ female teachers who should bloody well know better.
 Marcus Evans spoke to the Guardian in 2019 about concerns that a ‘gender-affirmative approach’ was being adopted by many school counsellors and CAMHS .
Marcus Evans spoke to the Guardian in 2019 about concerns that a ‘gender-affirmative approach’ was being adopted by many school counsellors and CAMHS .
“These parents all expressed alarm that, after their children suddenly announced they believed they were the wrong sex, practitioners were immediately endorsing the belief that this was the cause of the child’s distress, rather than offering time to explore perhaps long-standing psychological/developmental issues.”
Parents may have spoken to Mermaids, or Gendered Intelligence, or Allsorts, or other groups who make no secret of their support for puberty blockers.
Let’s presume the parent or parents are pretty sure their child isn’t actually suicidal. Nor do they believe blockers are the answer. They will still have to face down the teachers, friends, parents of friends and interfering aquaintences lining up to call their child by their new name and pronouns.That little ‘wokeamine’ hit can be very compelling.
 Parents will still have to worry about the ‘glitter family’ offered by the likes of Jeffery Marsh sinking their tendrils into their kids and telling them they’re ‘unsafe’ with their evil, transphobic parents.
Parents will still have to worry about the ‘glitter family’ offered by the likes of Jeffery Marsh sinking their tendrils into their kids and telling them they’re ‘unsafe’ with their evil, transphobic parents.
And if the fantasy is not indulged at home and the wrong tongues tell tattle tales, they may even find their trans-identified child removed from the family home and put in care.
Parents have all this to deal with. So let’s not be too hard on the parents.
Just stop
 While many people have been calling for trials into the efficacy and safety of puberty blockers, others have viewed the idea with alarm, and for good reason.
While many people have been calling for trials into the efficacy and safety of puberty blockers, others have viewed the idea with alarm, and for good reason.
In Newsweek, the Alliance Defending Freedom demands ‘Gender Medicine needs to stop treating young patients like guinea pigs’.
“…leaks confirm a massive scandal in the gender industry: many doctors prescribe hormones and perform surgeries on minors and vulnerable adults who are already beset with serious mental health issues while patients and parents don’t fully understand the risks and consequences.”
In Transgender Trend’s response to the consultation, they had this to say:
“We consider the risks of PSH used off-label for children too great to justify a clinical trial. We believe it is unethical to prevent a child’s natural pubertal development into adulthood, unless there are exceptional reasons for doing so, for example if the child’s condition is life-threatening. There is no evidence that medically preventing a child’s puberty is ‘lifesaving care’.”
What now?
There is a possibility that the research trials will not go ahead. There is even the possibility that it will become illegal to prescribe puberty blockers privately.
One of the main objections expressed concerning the provision of puberty blocker trials was that a research trial would be unethical. This could happen if it was decided that trials couldn’t adequately ensure the safety of participants.
The Public Consultation Analysis and Summary explains this well:
“Some… felt that the ethical aspects of the proposed research trial outlined in the interim clinical policy violated the 1964 Declaration of Helsinki by not adequately ensuring the safety and well-being of participants in the pursuit and development of medical knowledge and treatments, pointing to the Declaration’s 8th principle which emphasises that the primary purpose of medical research should not take precedence over the rights and interests of individual research subjects.
These respondents ‘requested an explanation of how the trial aligns with ethical principles to safeguard the rights and interests of the participating individuals and a clear rationale for using children as research subjects beyond advancing medical knowledge’.
Make it illegal
 Ex-Prime Minister Liz Truss called on MPs to back her amendment to the Health and Equality Acts Bill to extend the ban to private practices and make the prescription of ‘puberty blocking’ drugs to children completely illegal.
Ex-Prime Minister Liz Truss called on MPs to back her amendment to the Health and Equality Acts Bill to extend the ban to private practices and make the prescription of ‘puberty blocking’ drugs to children completely illegal.
However, on March 15th, when the bill could have been discussed in parliament, shadow defence minister Maria Eagle and others stalled for time, listing the names of pets and repeating the word ‘ferret’ until there was no time left to discuss the bill.
Truss was furious:
“Concerned parents will want to know why Labour don’t even want to discuss how to protect children and single sex spaces, let alone put those protections into law. Labour care more about ideology than the protection of children.”
Truss is supported by Kemi Badenoch, who blamed Labour MPs for the disruption, although others claimed that members of all parties were responsible. This ‘stalling’- more suited to a playgroup than a parliament- is a common tactic of MPs in this country when they wish to disadvantage discussion of a potential piece of legislation.
“Disgraceful to see MPs mocking the electorate, listing the names of their pets, in order to prevent the Health and Equality Acts private members’ Bill from being debated.” tweeted the LGB Alliance. “Puberty blockers are not a joke and this laughter is at the expense of, predominantly LGB, young people.”
“Riding off into the sunset, leaving ruin behind”.
On March 16th, the Times reported that staff at would receive generous payoffs as GIDS at the Tavi closed. Polly Carmichael, for example, will receive a juicy £80,000.
Transgender Trend called the payoffs “the final insult to medically damaged children & devastated families”.
Psychologist Dr Heather Wood, who was among those responsible for deciding which children got hormones and which didn’t, is reported to have gone travelling with her payoff.
The Times revealed that Wood had previously posted on social media that gender-critical feminists were ‘like racists’, single-sex spaces ‘like apartheid’, and that she referred to the Bayswater Suport Group, run by the concerned parents of trans-identified children, as ‘transphobic’.
 Staff once raised concerns with managers at GIDS in Leeds, after Wood speculated that a girls’ interest in a Thomas the Tank Engine toy meant she might be a good candidate for puberty blockers.
Staff once raised concerns with managers at GIDS in Leeds, after Wood speculated that a girls’ interest in a Thomas the Tank Engine toy meant she might be a good candidate for puberty blockers.
 Wood recently posted on facebook that she’s off on ‘a wee road trip’ at the end of March, and guess what she plans to do on her return?
Wood recently posted on facebook that she’s off on ‘a wee road trip’ at the end of March, and guess what she plans to do on her return?
Open a private practice!
Possibly even run it from the back of her campervan.
It’s all about the ‘trans kids’, after all.
