 The ‘Women Create’ conference was the brainchild of Victoria Gugenheim and featured forty eight female artists from around the globe. Responsible for the overall curation, Victoria structured the panels and approached many of the artists. Her focus was on performance and activist art, whereas Claudia Clare was responsible for the upstairs curation and for ensuring the exhibition featured a balance of museum and gallery artists alongside ‘grass roots’ creatives.
The ‘Women Create’ conference was the brainchild of Victoria Gugenheim and featured forty eight female artists from around the globe. Responsible for the overall curation, Victoria structured the panels and approached many of the artists. Her focus was on performance and activist art, whereas Claudia Clare was responsible for the upstairs curation and for ensuring the exhibition featured a balance of museum and gallery artists alongside ‘grass roots’ creatives.
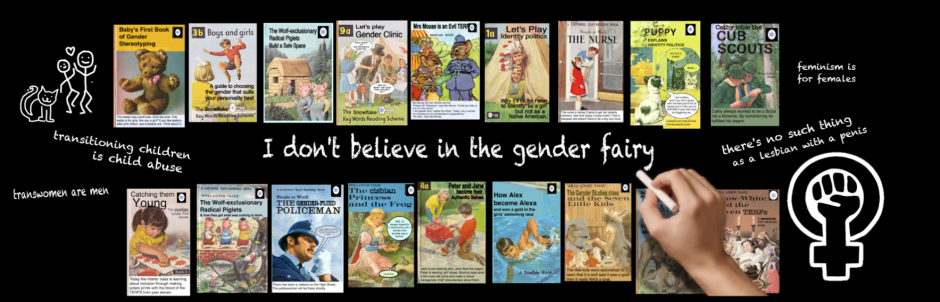
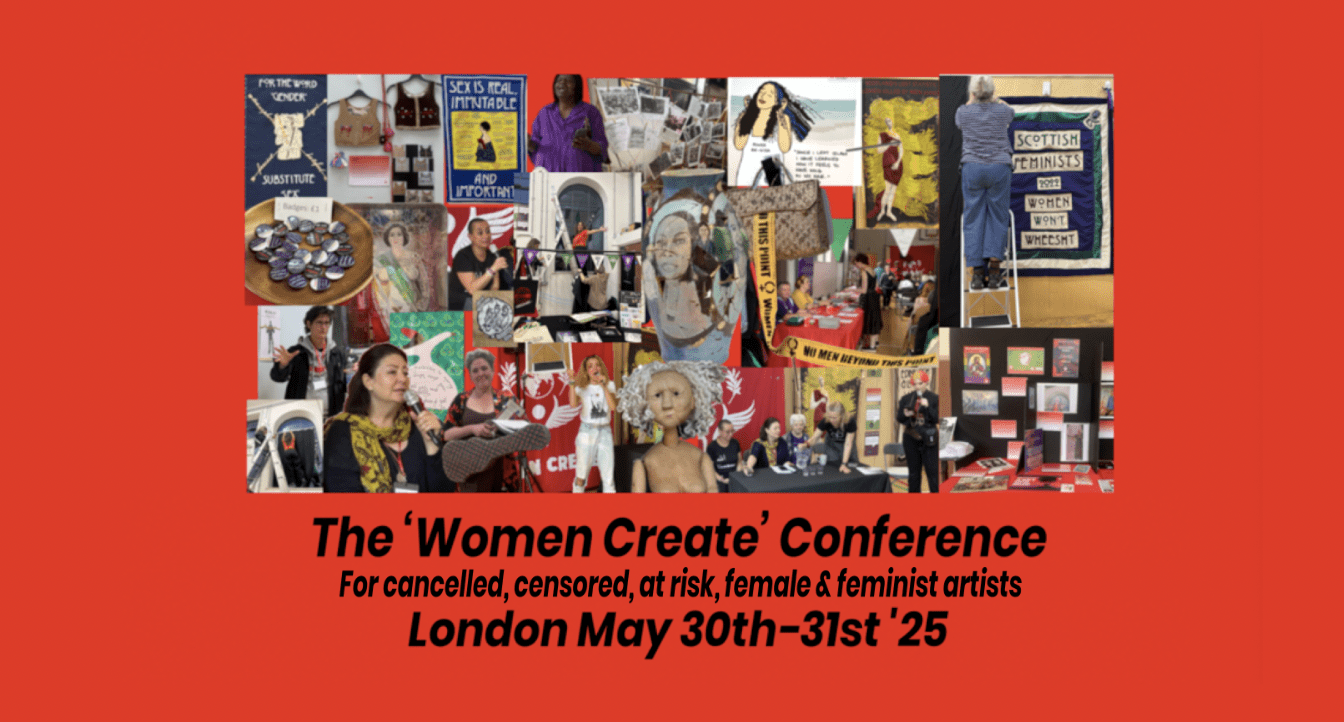
Described as “the world’s first ever event platforming cancelled, censored and at-risk female and feminist artists”, it took place over two days, in North London on May 30th and 31st 2025. I was chuffed to be invited to come along, to write about and photograph the event, and to bring my ‘Gilding the Lily’ stall.
I wasn’t able to see everything, as I had a prior engagement on Saturday, but I’ve tried to give an idea of some of the beautiful and inspiring work on show. I’ve interspersed my précis of the discussion panels with photos and details of the artworks exhibited upstairs. All photos are my own.
You can see the full program here.
Setting it up
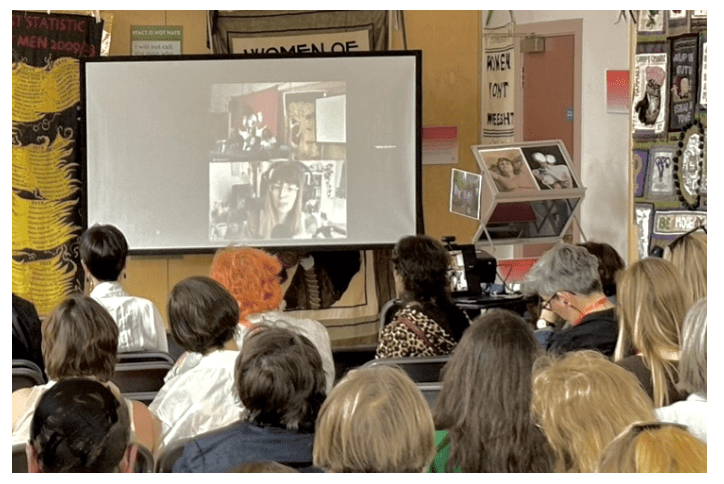
We had been allocated several hours on the Thursday evening to set everything up, and things were predictably chaotic. One of the more Sisyphean tasks was trying to attach dark curtains and posters to the large arched windows of the main hall. Some of the panels were using projectors, and a film, Vaishnavi Sundar’s ‘Behind the Looking Glass’, was to be shown in the main hall on Saturday.
The organisers had been told, with only a few weeks to go, that they wouldn’t be allowed to put up proper blackout blinds, so we were doing the best we could. We stuck our curtains up, they fell down. We stuck them up again, they fell down again. Talk about tubthumping. We put them up again. We were unfazed by their lack of co-operation. We were having an art event and it was going to be amazing!
You can view the full program for ‘Women Create’ here.
My stall was established in a corner by the main door, near the registration desk and the Nordic Model Now stand, and eventually things were as ready as they were ever going to be. Most of us left with plans to get some sleep and return less than 12 hours later. Others (ahem Kelly & Shabanna we see you) went to the pub. Victoria was still adding the finishing touches as we left- I don’t think she got very much sleep!
Friday morning
The next morning we were back at the venue bright and early. It was a hot sunny day, and when I arrived at 9.30, the stewards were already set up outside in a splash of purple colour. At ten o’clock, attendees began to arrive for registration. It was a relief to have done all my unpacking and arranging the night before and to just sidle into place with a flask of coffee and watch things unfold around me.
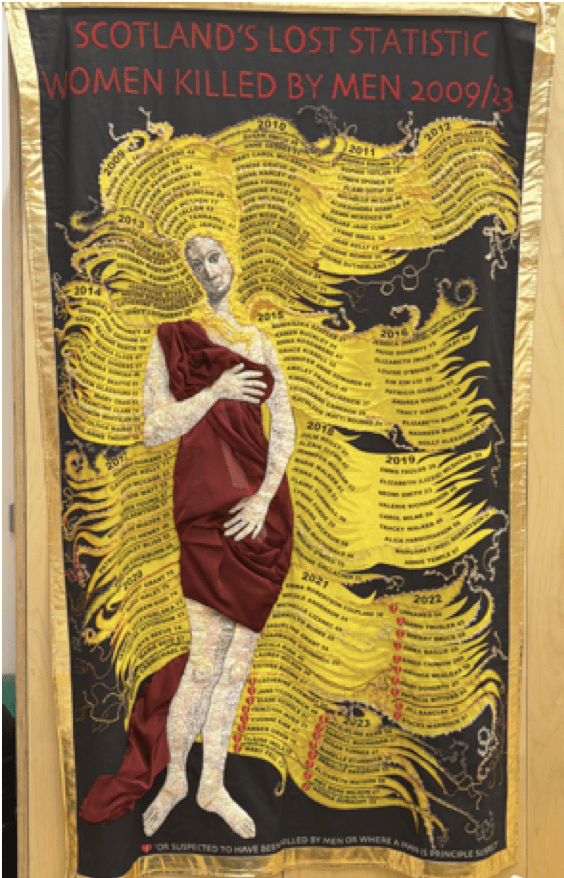
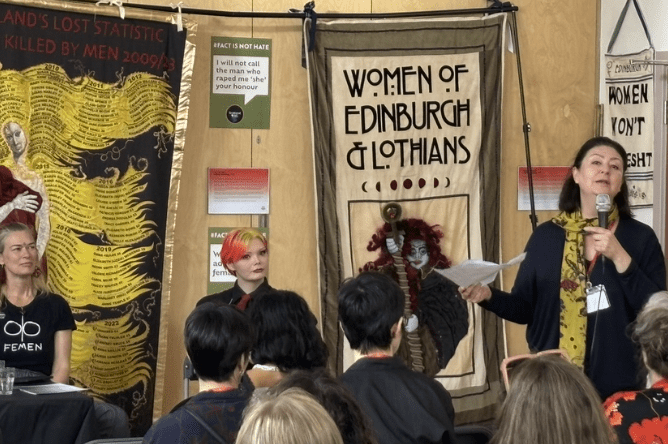
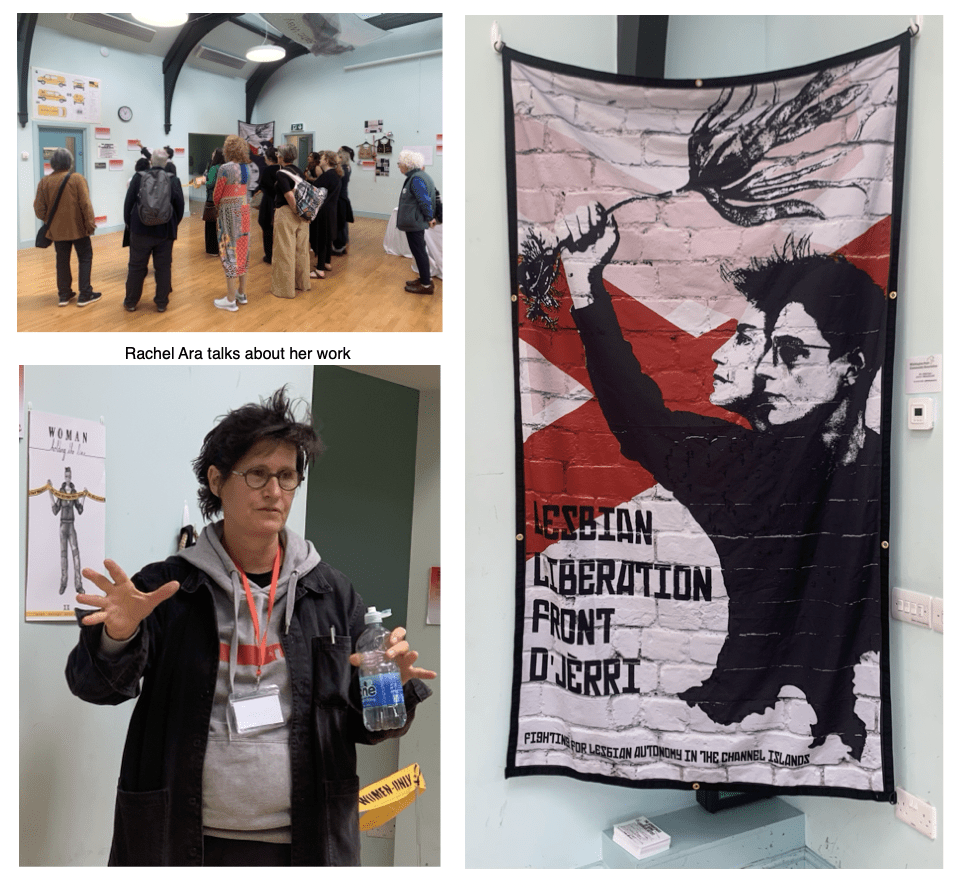
While we waited for the first panel to begin, many admired the beautiful banners which adorned the walls of the hall. Jenny Reilly creates banners for the Scottish Women’s Rights group, Women Won’t Wheesht.
These really have to be seen to be appreciated. Created with a mixture embroidery, appliquéand felting, often featuring intricate details that need to be viewed with the naked eye.
I especially liked the Selkies’ kitten in a pussy hat. I couldn’t get my mouth around the phrase, ‘a tup in a tutu isnae a yowe’, even after Lorraine- described by a fellow Selkie as “our most gifted and hilarious textile artist, by a country mile,”- repeated it several times for me.
The Selkies aim to create banners that will be featured in the museums of the future. The collective skill, humour and attention to detail is impressive. Hopefully the museums of the future will be appreciative!
I checked out the stands next to my stall and watched the gathering women as they chose seats and prepared for the first panel.
Things were running a little late, but attendees were still arriving. My mum was helping me with the stall, so I could scoot off and take photos, and we had a perfect view of the proceedings.
I decided to listen to the first panel before perusing the work upstairs.
“Playing small doesn’t save the world,” said Victoria, in her introduction.
“You cannot have a revolution without sparking joy; we are that joy. You cannot have a revolution without changing the culture; we are that culture!”
The first panel
We are women, our bodies cannot be cancelled
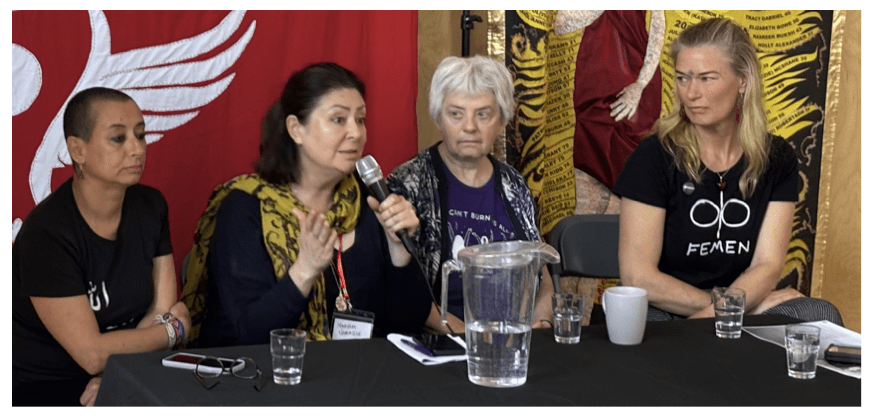
Left to right: Betty Lachgar (M.A.L.I), Maryam Namazie (Council of Ex Muslims of Britain), Ray Raymond (Greenham Women Everywhere), Jenny Wenhammar (FEMEN), Victoria Gugenheim
The panel was chaired by Victoria, who has worked as a core artist with the Council of Ex-Muslims, and been involved in topless protest with FEMEN. Each speaker was allocated ten minutes to talk, and the talks were followed by a Q&A.
Jill ‘Ray’ Raymond, from Greenham Women Everywhere
Ray observed that she had no powerpoint or notes, but she did have a lot to say. Greenham has been erased from feminist history, she told us, but she and others have been able to undo this omission.
Recently some women had managed to acquire funding to set up Greenham Women Everywhere and archive Greenham’s oral history. Reminding us that there was no social media back in the 1980s, she added, “It has just been fantastic to interview women and go around the country”.
Raymond said she had a particular interest in telling younger people about Greenham, “as they seem to think that the suffragettes were the last big struggle for women”.
Greenham Common Women’s Camp was an international two year protest, aiming to prevent American nuclear missiles from being sited just outside London near Reading. Initially Greenham was a march from Cardiff, with plans to stay for a just few days. At the start there had been some men present but they soon left the camp. “They were a pain in the arse and didn’t do their washing up,” she joked.
The second year, 1982, 30,000 women turned up at Greenham. “There was a nine mile perimeter fence around Greenham and we did a women-only holding hands around that nine mile fence.”
More and more camps were established at Greenham over time, and women stayed for longer and longer. Some brought their children, and one woman gave birth in a teepee in the woods. Many of them did not want to return to the lives they had before. The first day of the ’embrace the base’ protest was peaceful with lots of singing and chanting. This was disparagingly referred to as “grannies for peace” in the press. The second day the women instigated a blockade.
“Once we actually started putting our bodies on the line… 30, 40 or 50 women lying in front of the gate, huge convoys of American military trucks… they were dragging us off… one of the ways we made it difficult for them was to weave webs of wool. We put webs on the fence but also used them for blockading.”
Raymond gives an example of the way they would use these webs. Hundreds of women were being arrested, so the courts started trying women in their home town magistrates courts. Three women took balls of wool into Totness Magistrates Court and ‘webbed up’ the public gallery.
“They couldn’t throw us out because they couldn’t get us out of the webs,” she told us. “They had to send the steward out to buy some scissors!”
Greenham Common Missile Base is now a wildlife haven, home to protected birds, rare plants and over 30 species of butterfly.
Betty Lachgar of Mouvement Alternatif pour les Libertés Individuelles (MALI)
The next speaker, Betty Lachgar, began by telling us that her T-shirt read ‘Allah is a lesbian’. After wearing it at a conference in Germany in 2020, she was arrested on her return to Morocco. The investigation is still in progress.
She explained a little about the position of women in Morocco, an absolute monarchy where everyone is Muslim. Betty is an atheist but “in Morocco this was not possible”.
Morrocco has a Penal Code and a Family Code. The Penal Code controls sexual and reproductive rights, especially those of women, for example sexual relations are prohibited outside of marriage, adultery is criminalised and abortion is prohibited. Homosexuality is punishable by imprisonment and lesbian women are often married off by force. The family code is based on Islamic laws and reduces women and mothers to the property of men, where they are relegated to the private sphere as domestic and sexual slaves.
“The family code is inspired by religious texts and men have the legal right to dominate and oppress women.”
She gave examples: the marriage of underage girls, polygamy, and “dowry, which is a form of prostitution”. Unmarried mothers are considered equal to prostitutes and their children are illegitimate in law. “The family code is written by men for men.”
Betty has founded Mouvement Alternatif pour les Libertés Individuelles (MALI) a movement of civil disobedience to fight for freedom of speech, freedom of conscience and women’s rights. “We denounce and condemn male and sex-based violence.”
The group organises events and ‘provocative actions’ and aims to break taboos on sensitive subjects, taking the streets and public places for women and making them our own. She says this has not been easy, but it has resulted in her travelling around the world, “meeting amazing feminists, and fighting with them”.
In 2016 Betty was sexually assaulted by police officers in police custody because she had hidden her phone under her breasts. After one of them told her, “at least we’ve seen your vulva and vagina,” she received a one month suspended sentence for assaulting a police officer.
Maryam Namazie from the Council of Ex-Muslims of Britain
Maryam Namazie from the Council of Ex-Muslims of Britain was our next speaker. There were some difficulties viewing the powerpoint as the large windows allowed so much light. This meant it was hard to see many of her slides.
Topless protest is often thought of as being a western form of resistance, she told us, but there is a history of naked protests in many other regions including Nigeria, Kenya and the Middle East. After Tunisian Amina Tyler posted a topless photo of herself online in 2013, with the phrase “my body is my own” scrawled across it, she had to go into hiding and calls were made for her stoning.
Maryam spoke of the ‘woman life freedom’ movement in Iran, saying, ‘you cannot free a society without freeing women’. Of her own activism, she mentioned a protest in front of the Louvre where she cut out the word ‘Allah’ from an Islamic flag and replaced it with a picture of her vulva.
The slideshow Maryam had prepared included images of naked and undressed women using their bodies to protest, as she reminded us that in Iran even not wearing a veil can result in ten years in prison.
“The hair is an extension of the body, and the body is an important site for resistance because it is the battleground for oppression and exploitation.”
While women’s bodies have always been exploited, Maryam believes we are entering a new phase with the rise of the religious right and patriarchal systems of global oppression. Maryam views topless and nude protest as a radical act of reclaiming bodily autonomy and challenging the systems that seek to discipline and exploit women. She concluded by reminding us that women’s bodies can serve as a powerful symbol of resistance against oppressive forces.
Jenny Wenhammar of FEMEN
Jenny was raised in Sweden by a mother who used to walk the dogs topless in the nearby forest. Her first topless protest was at FEMEN’s ‘topless jihad’ for Amina in 2013. It was ‘amazing’ to feel the wind, not only in her hair -which of course is also banned for many women- but on her breasts, in a way that feels very different from topless sunbathing. Men walk around topless all the time, of course, ‘but this experience is denied us because we are women’.
Femen was an organisation started in Ukraine in 2009, by Ukranian women, in protest against women being seen as objects and sold in the sex trade. It also stands against dictatorship and theocracy.
Describing herself as ‘a very agreeable person’, Jenny notes that she has been repeatedly cancelled because of her work with FEMEN.
Despite her previous position as a Green Party politician, it was initially hard for her to leave the niceness behind and instead shout – she screams – “Fuck you!” and be unashamed to take up space.
FEMEN was once on the list of organisations considered to be a threat against the Russian Motherland, and Jenny says ‘there are a lot of lies’ that have been told about them.
She recommended that people with questions talk to members of FEMEN, who are always willing to answer any questions about the organisation. Wenhammer herself answered questions in the Q&A following the talk, including countering the idea that FEMEN is or was run by men.
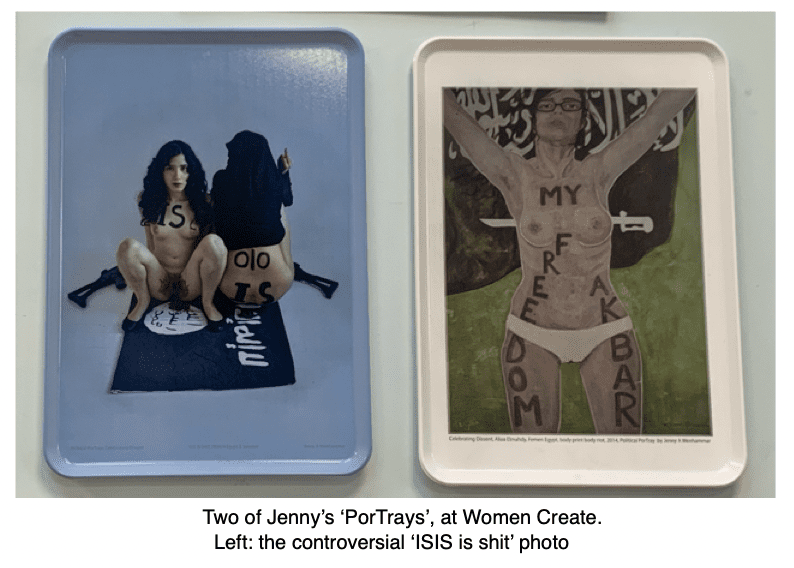
Her own art consists of photographs or protest and portraits of FEMEN activists, and is seen as highly controversial.
In 2014, she tells us, she made an ISIS flag, and she and another woman were photographed menstruating and defecating on it. She has been in court several times for her feminist actions.
Denmark as a very liberal country, and one where pornography is popular, yet Jenny has been put on trial there for indecency- for going topless. She calls this a ‘huge hypocracy’ and speaks of the deplatforming and threats from the Christian and Islamic far right. While acknowledging her privilege compared to women in many parts of the world, she has lost her home, her house, her health has been affected, and she worries for her family. Despite this, she maintains a positive attitude.When Jenny finished, Victoria thanked the speakers and asked us to give a cheer for Claudia Clare, “who has worked so to bring all these artists together under one roof.” Claudia was upstairs so she didn’t hear us, but we definitely cheered!
Lunchtime & the Mysterious Fire Alarm
The organisers had been told by the centre manager that the venue’s cafe would be open for attendees to purchase lunch, and this had been mentioned in the program, so we were surprised and disappointed to find it closed. The High Street was a short walk away through the park but there was nowhere closer to buy food or drink, although organisers did provide tea, coffee and snacks. This caused problems for many attendees; some left it too late to go for lunch, some skipped lunch altogether, and more than one woman with health issues had to miss the afternoon sessions because the promised cafe was closed and she needed to eat on site. Others were late returning to the afternoon session, which was promptly and mysteriously interrupted by a fire alarm in the middle of Nehanda’s act. But more of that later.
The venue- which had originally tried to cancel the event on the grounds that some artists were ‘transphobic’- was not forthcoming with an explanation as to why they had not informed organisers of the sudden change of plan.
After eating my packed lunch & chugging some coffee, I had just enough time left to nip upstairs and look at a couple of the pieces on display, something I would do throughout the day.
A detailed tour of the works on the upper floor, led by Claudia Clare, took place at lunchtime and I briefly joined. I’d love to have had time to analyse all the artwork in detail, but I’ll share my observations briefly. Apologies for the pieces I missed.
Rachel Ara, & Angela Wild
We looked at Rachel Ara‘s work, with a short talk from the artist. Ara’s work explores “relationships between sex, gender, technology and systems of power.” During the COVID lockdowns, Ara turned her van into a mobile art exhibit with ’24 Hour Merntal Breakdown Service’ written along the side. Sightings went viral on social media. You can learn more about Outrageous Algorithms (A fourth emergency service for todays problems) here.
.Rachel has worked collaboratively with Angela Wild, whose performance art piece ‘No Men Beyond This Point’ was also featured in the exhibition. The piece consistes of a handbag, designed to contain six retractable poles and concrete bases, and a ‘police tape’-style ribbon reading “Women Only – No Men Beyond This Point”.
“By placing a boundary around us and restricting entry to women alone, we place a symbolic boundary around us AND around the definition of woman.” says Wild. “Without a clear definition of ‘woman’ there is no feminism, no sex-based rights… Definitions are linguistic boundaries… Apples aren’t oranges… People who insist that men can be women often accuse us of gatekeeping the word “woman”. Indeed, this is what we are doing.”
Victoria Gugenheim
Victoria was exhibiting her piece ‘My Big Fuck Off Bush”.
The exhibit, described as “A fun, punny play on defiance of gender norms and female intimate body hair” literally lit up the room, as she had woven fairy lights into the plastic foliage.
“”This was originally aired on Beyond Gender with Stella O Malley as my backdrop,” she told me. “It’s my pride and joy- because every lesbian needs a big Fuck Off Bush. I even gave it a LED jazzle for its exhibition debut! Remember, you can only touch my bush if you ask nicely and I say yes. Don’t touch anyone’s bush without their permission!”
Fanny Graham (Tiny Haunts)
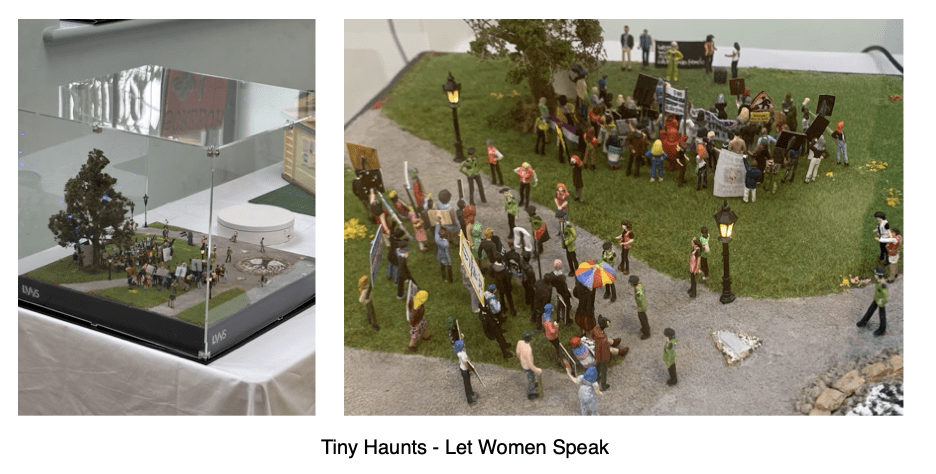
Fanny Graham‘s miniature re-creation of a Let Women Speak meeting in London’s Hyde Park was fascinating.
Fanny’s piece “features recognisable banners and figures, both famous and infamous, from real LWS events across the UK” and addresses “the broader tensions surrounding this political movement and free speech in public spaces today”.
She had really captured the feel of it, even including the Reformers Tree mosaic, the vintage streetlights, and the angry TRAs. I loved the way you can see the stewards holding the line. There was a magnifying glass next to the case for those who wanted to take a closer look.Graham writes that she wanted “to honour the courage, solidarity and defiance of women who stand tall and speak the truth despite immense intimidation from misogynist men and their handmaidens… small figures, big voices.. tiny worlds.. powerful truths and art that holds the line.”
Sarah Lawson
A series of miniatures, titled “We get on like a house on fire,” pretty well speaks for itself. Very dark.
BigMumma
‘Tale from Taliban High’ features Sylvanian family dolls dressed in blue cotton burquas, a piece created by a woman calling herself BigMumma.
School books litter the floor and chairs are overturned. The girls are banished from the classroom, eyes raised to the viewer.
My kids loved Sylvanian Family toys when they were little, cute little anthropomorphised wildlife critters whose adventures were only constrained by imagination. The fantasy world these creatures embrace is in stark contrast to the reality facing girls deprived of an education and numerous other freedoms.
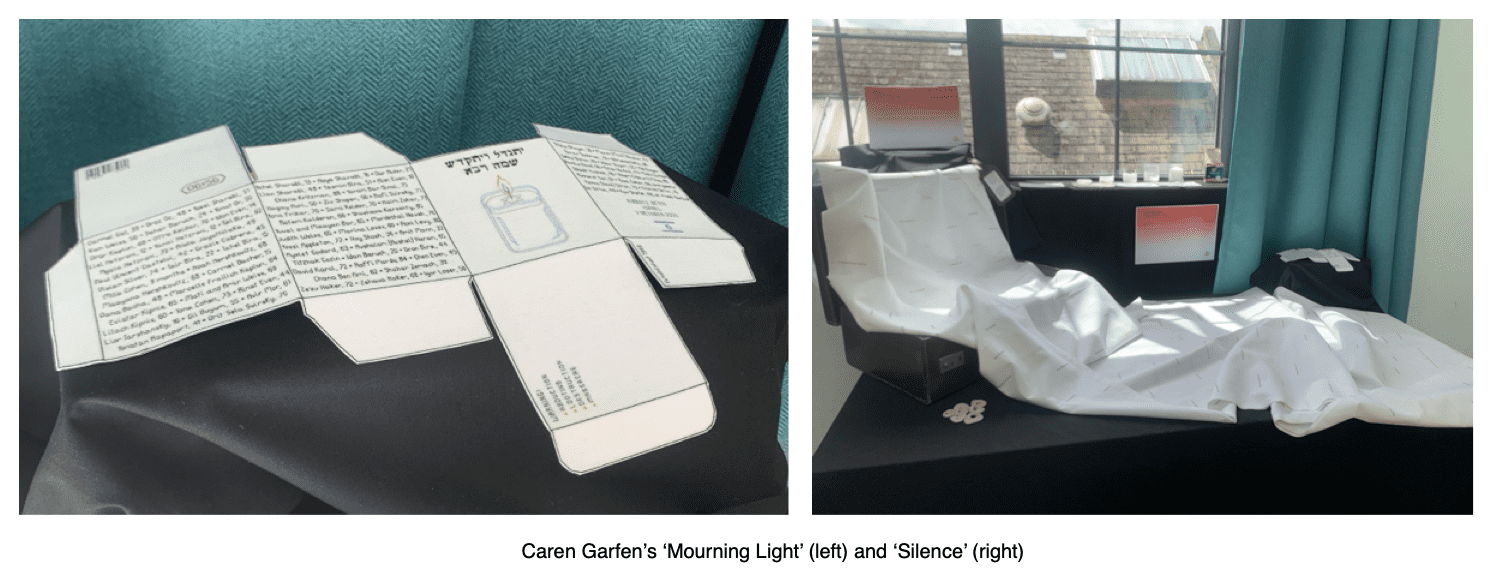
Caren Garfen
I was moved by Caren Garfen‘s ‘Morning Light’, a recreated remembrance candle box, featuring the hand-stitched names of the 101 people murdered at Kibbutz Be’eri in Israel on October 7th 2023. It was exhibited next to her shroud, stitched with the names of women raped and murdered by Hamas terrorists on the same day.
A sober thought. Lunchtime was ending, so I headed back downstairs to the main hall.
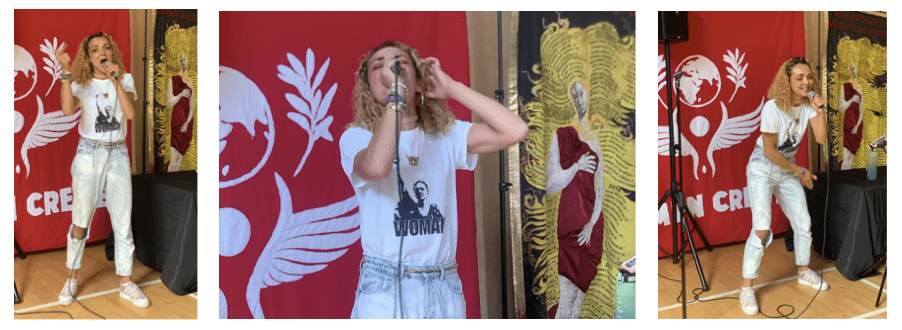
Nehanda Music
It was time to listen to some music from Birmingham artist, the fabulous Nehanda Music. Her music has a hip-hop feel with a sprinkle of rap- very upbeat, and I liked both her energy and her voice. She was about ten minutes into her set – Kelly and Victoria were dancing at the back and I was contemplating joining in- when suddenly there was a hideous cacophany drowning out the music- the fire alarm going off.
Outside we traipsed. It was bloody annoying. We never received any clarification as to why it might have happened. In the light of the closed cafe, and a few other incidents that seemed specifically contrived to blight us, one might have been forgiven for suspecting that somebody was trying to cancel the cancelled women.
This idea gained further plausibility when those going to buy tickets online on Saturday morning found that Eventbrite had listed the event as ‘postponed’.
But it would take more than a fire alarm to dampen our spirits! A register was taken, we were all present and correct, and normal service was resumed. As you can imagine, this cut into our conference time, but it was a sunny afternoon and we were undaunted. Back into the hall we piled for the next panel.
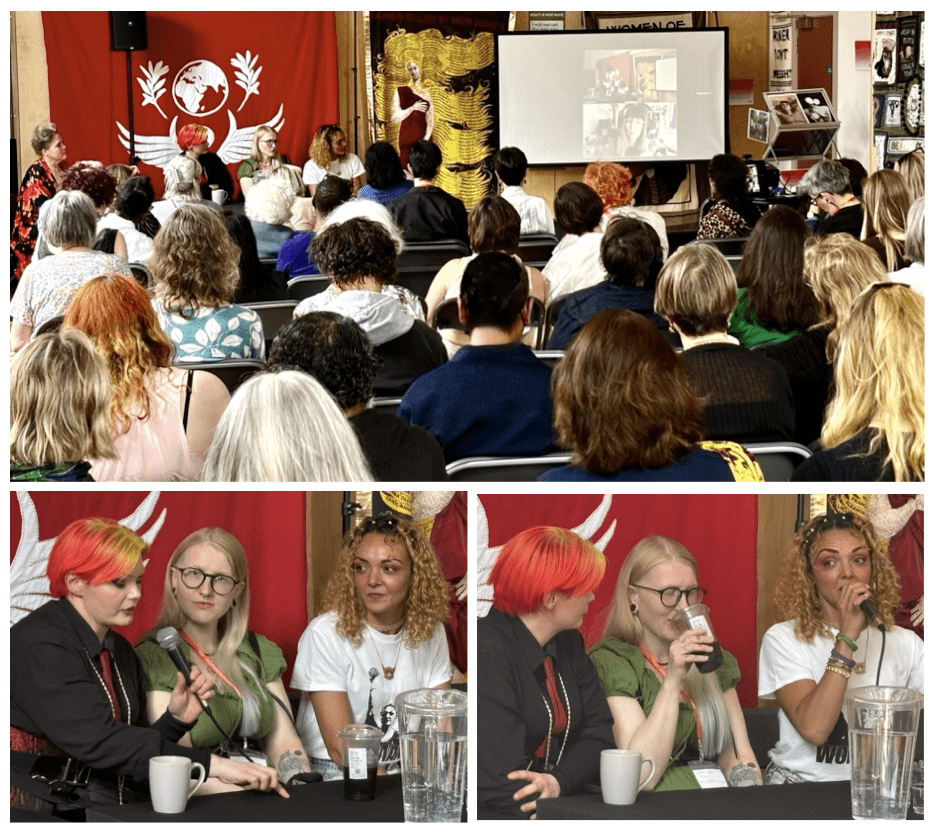
The second panel
Aesthetic Policing, Survivorship & Self Expression in Women’s Movements
Elly Arrow, Genevieve Moon, Nehanda Music and Victoria Gugenheim
Rebecca Mordan, artistic director of ‘Scary Little Girls‘, stepped in to chair and introduce the panel members.
Victoria Gugenheim
After attending a major women’s conference in 2022, Victoria realised that while many feminists were approachable and nonjudgemental, others could be brutally disparaging about the way she chose to present herself, with bright clothes, hair and make up. It felt pertinent for her, as a detransitioner, that such diversity was seen as suspicious within the movement. “If you like anything that’s a little bit alternative you are not given sisterhood.”
The social media algorithm is not conducive to sisterhood, says Victoria, geared as it is towards encouraging individuals to behave aggressively towards each other. Victoria believes that the ‘social policing instinct’ is one of the things that lets the feminist movement down. Many women use bright make up or clothing as a way of asserting themselves or taking up space. She herself has been criticised by women for the way she dresses, and accused of pandering to the male gaze. Such policing of women’s behaviour, clothing and speech, she says, creates a cultural form of coercive control. Two women she knows have ‘returned to the BDSM scene’, where she worries for their safety, after being overtly criticised by feminists for their clothing or hair and make-up choices.
“I think it’s a crying shame- and a massive assumption- that just because somebody likes a bit of aesthetic adornment that they’re ‘doing it for the menz’… I don’t care what you’re wearing, I don’t care about your haircut, I care about you having investing thought and opinion; I care about what you have to say; I care about what you bring to the table and I care about your art… Women Create is that culture.”
Genevieve Moon
Genevieve introduced herself as “a serial abusive survivor and radical feminist”. She first came to radical feminism through Twitter but was bullied from the platform by other women. Her username, ‘rad femme Barbie’, she thought was funny but certain elements did not. She was accused of dumbing herself down and trying to ‘make herself appealing to men’.
Moon acknowledges that ‘gossip’ can be used by women as a tool of survival, but also observes that women can use it to drag other women down.
“We talk amongst ourselves about the dangers that we face, we talk about the strange men we meet, and it helps us stay alive as well. Women, in a way, are natural prey to the human male.”
When she announced her pregnancy online, Genevieve was subject to bullying from other women, including being asked, ‘are you having a girl or are you having an a-boy-tion?’ After giving birth to a baby boy, she says she received death threats, and her photos were shared online by women saying they hoped her baby was sexually assaulted or killed.
“Monkeys gang up on each other,” she observes of some online communities. “People will drag up a screenshot from ten years ago… if it wasn’t for actual real life connections with activists I would simply have not been in the movement anymore and it’s not for a lack of belief, or a lack of wanting change.”
Nehanda Music
Nehanda said she’s never faced aesthetic policing herself, possibly because she’s never labeled herself as a feminist, despite holding radical feminist views. Growing up,she said “everything I know about feminism had come through my mum and if I’m very honest it seemed very boring and I wanted nothing to do with it.”
Her family’s black culture, rooted in Trinidad, deeply influenced her growing up. ‘Part black’ she was raised in a black family where a great deal of emphassis was placed on black identity, especially by her father. After moving away from her dad, as an adult in England, paler-skinned herself, she wrestled with identity: “Something in my head was saying ‘oh, maybe you should cornrow your hair, and you should do this…’
Nehanda feels she’d be cancelled for calling herself a black woman, despite her background. So she was baffled when it became clear that that men can identify as women without similar scrutiny. Suddenly, “everything my mum told me fell into place.”
When she first began attending radical feminist events she noticed that many of the women reminded her of her own mother’s style of dress, little or no make up and plain clothing, and she found herself mimicking this style despite it not being her own. She was happy to meet Victoria, who had her own unusual style, and it made her realise it was ok to express herself. She concluded that there should be room for all women within feminsm.
Elly Arrow
Elly Arrow joined the group by livestream from Germany.
“Thank you all so much for having me. I hope there’ll be many future Women Create events where I can actually see all of you in person, and thank you for the opportunity to exhibit some of my work. I felt it wasn’t good enough and it means a lot for women to say yes it is.”
Having spent eight years in Germany’s movement against commercial sexual exploitation, though not a survivor herself, she has seen its impact on women’s lives, and as she reminds us, “all of us live with the men who so enthusiastically use these industries.”
It is a world, she says, encompassing femicide, early death, slow death and trauma.
“A lot of people calling themselves allies have really rigid high expectations of women who have left prostitution,” she tells us. They hold strict ideas about what women should wear, and how they should look, having exited the industry. They aren’t expected to have ambiguous feelings about their experiences, and they are frowned upon if they dress in a way which might be considered designed to appeal to men. Women willing to appear on television or in photos in the papers are criticised viciously in the comments sections, by women who call themselves allies, often in a way that purports to express concern but is dripping with judgement. The reward for their bravery at a time of vulnerability is these cruel comments.
“We’re calling women ‘too whoreish’ to be taken seriously, that’s what we’re saying a lot of the time, and women are hearing this, women who’ve come out of the industry.”
Survivors have enough to worry about and critiques about appearance are not supportive. Women still in the sex industry face similar attacks on their appearance, judged for skimpy clothing, plastic surgery and prolific make up, and survivors see this. The fight should be against those profiting from women’s exploitation. Survivors and women still within the industry deserve space to be themselves without judgment from those who clalim to be their allies Our focus should stay on dismantling systems of abuse and oppression, not judging the women entangled within them.
You can read Elly Arrow’s 2024 piece ‘If I was a prostitution survivor, I wouldn’t tell you’, here.
The session was followed by a Q&A.
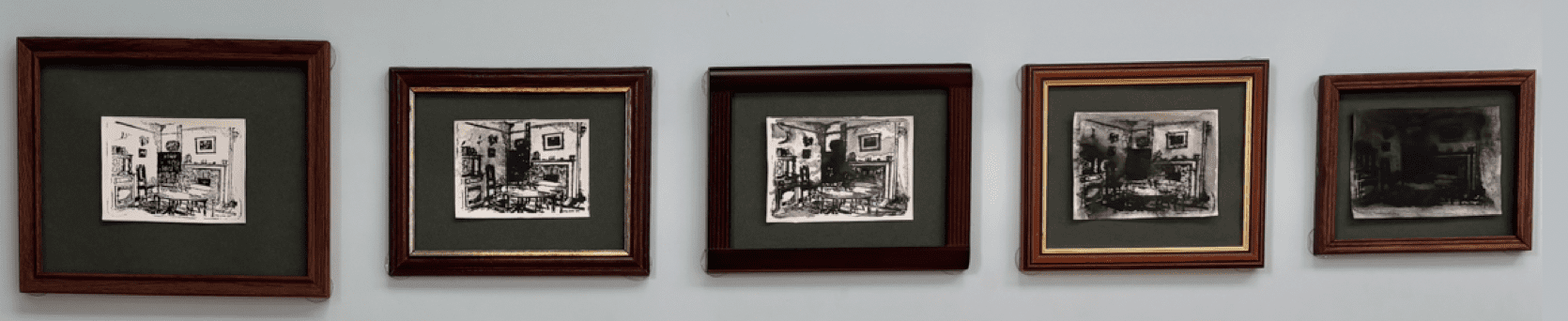
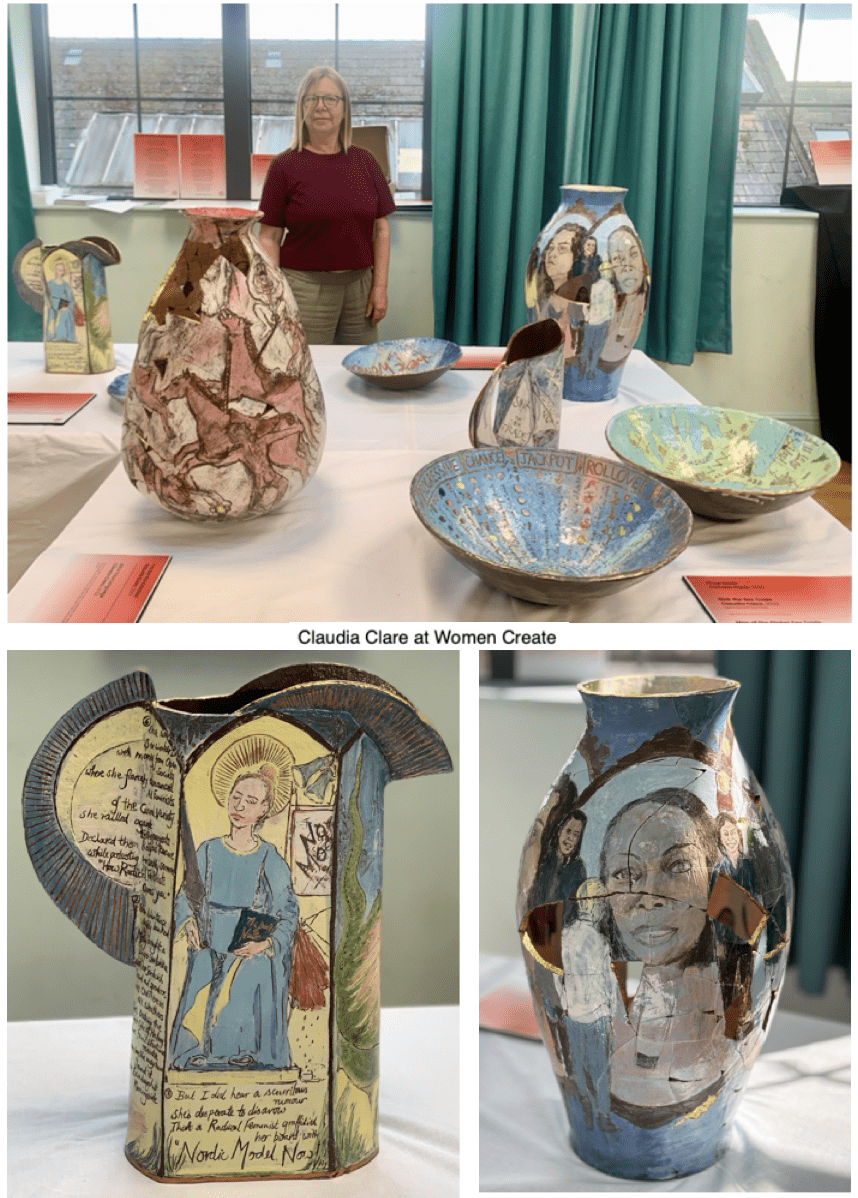
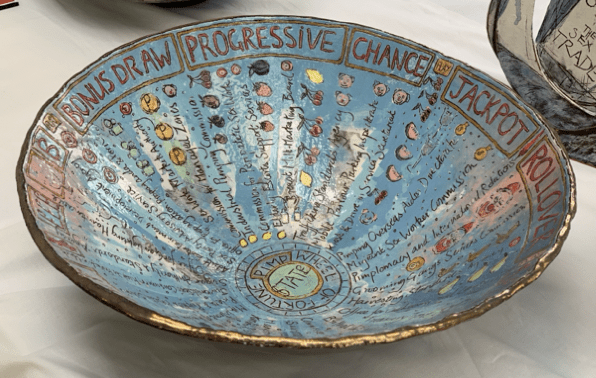
Claudia Clare
Claudia Clare creates painted pots with elaborate images and text, sometimes broken and recreated, always telling a story and provoking feminist thought. Her bowls feature text from sex trade survivors; the bowl on the right (centre) charts a map of the global sex trade.
“Astonishingly, none of the work I did with women in the sex trade has been shown in a public gallery in the UK, because I am a sex trade abolitionist.” Clare told me.
“This was a ticketed event, so still not really a public space, even though it was in a community centre. Displays, exhibitions and lectures about this work have been cancelled repeatedly. It has been, and is still, immensely frustrating.”
“That said, it was an excellent space for pots because the light was so good, and many people saw the work and had a chance to talk to me about it.”
Clare was also curator for the upstairs floors at the conference, which she originally doubted would come to fruition.
“I was initially absurdly relaxed about being the curator because I honestly didn’t think we were going to get a venue! Within the ‘cancelled artist’ circles we had been talking for at least four years now about having a conference, or having an exhibition, and I had pretty much resigned myself to the idea that it wasn’t going to happen.”
Claudia says she was impressed by the scope and depth of Victoria’s vision. Where Claudia had initially imagined a few women renting a room over a pub; Victoria envisioned ‘Women Create’ eventually growing into a vast festival.
“I really didn’t think it would be possible,” said Claudia, “But Victoria really has pulled it off!”
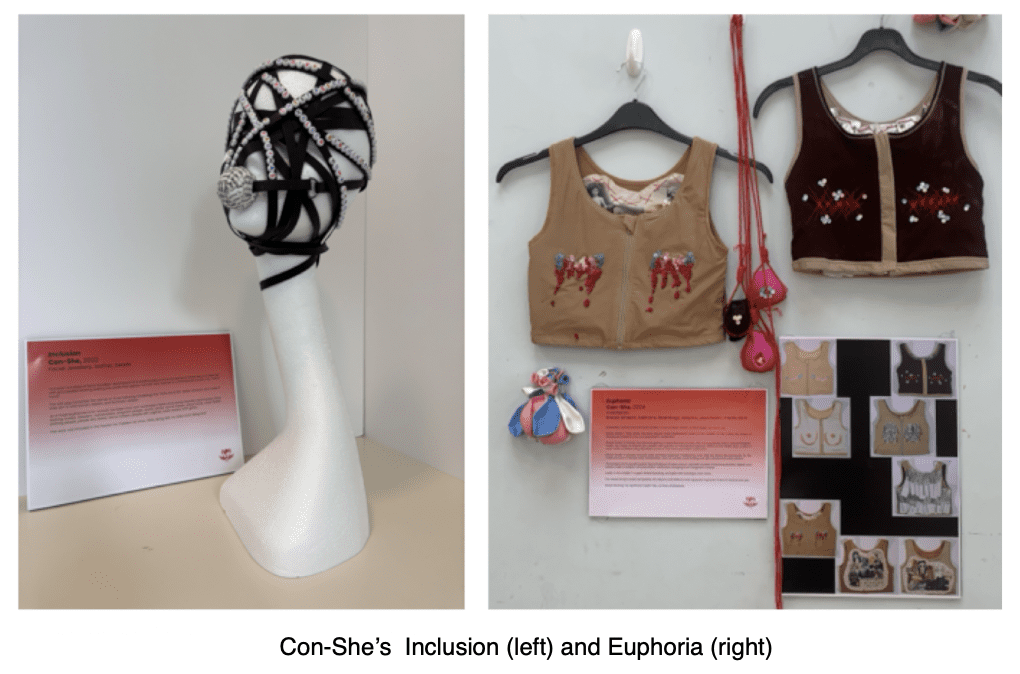
Con-She
Anonymous artist Con-she‘s visually striking work is always powerful. At Women Create she exhibited several pieces, including one of my favourites: Inclusion, a piece of ‘facial jewellery’ reminiscent of a ‘scold’s bride’, used to silence ‘gobby’ women in years gone by, but with a modern ‘bondage’ twist.
Of her breast-binder installation, ‘Euphoria’, she writes, “The whole thing is sordid and joyless, the sequins and balloons and supposed euphoria a kind of visceral sick joke.”
After the conference, Con-She told me, “Women Create was a really groundbreaking event! Incredible artwork that, sadly, doesn’t otherwise get shown. Inspiring speakers. And, by and large, a spirit of tolerance for disparate viewpoints. It really felt like part of a groundswell – finally a movement coalescing.”
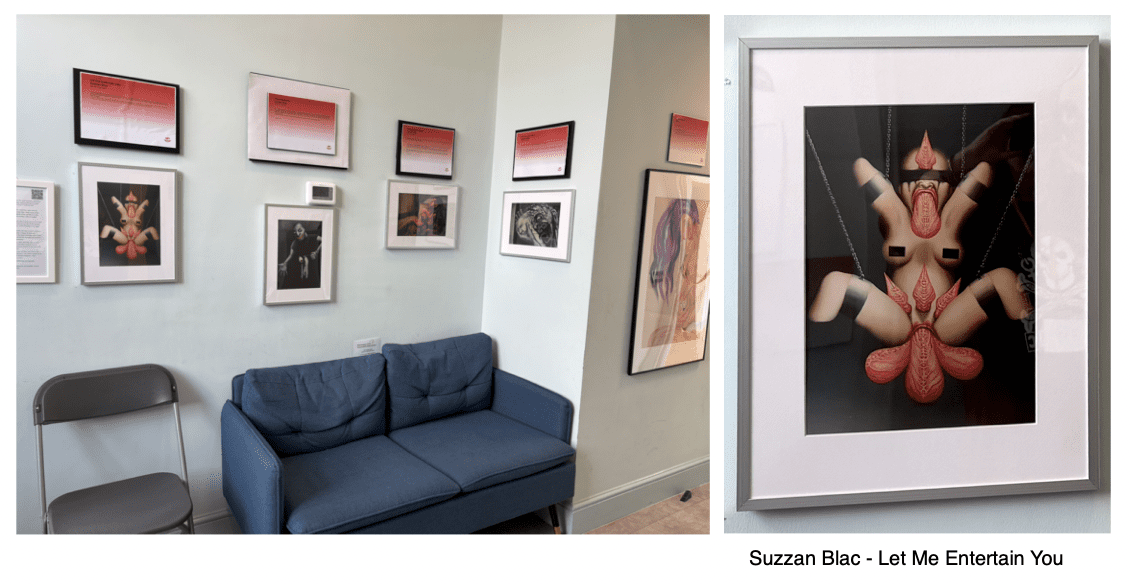
Suzzan Blac
In a bright lit, wide hallway at the top of the stairs perched a comfortable sofa and around it hung some extrememy uncomfortable images. Suzzan Blac’s raw, gut-punching and evocative work chronicles her traumatic journey through a young life of sexual abuse and exploitation.
Of her paintings, Blac writes, “In 2011 I decided to put them online. I had other works out there, but I knew that silence ‘impairs the victims and empowers the perpetrators’. So I had to speak out…”
My photos of the images do not do them justice. You can see and read more here.
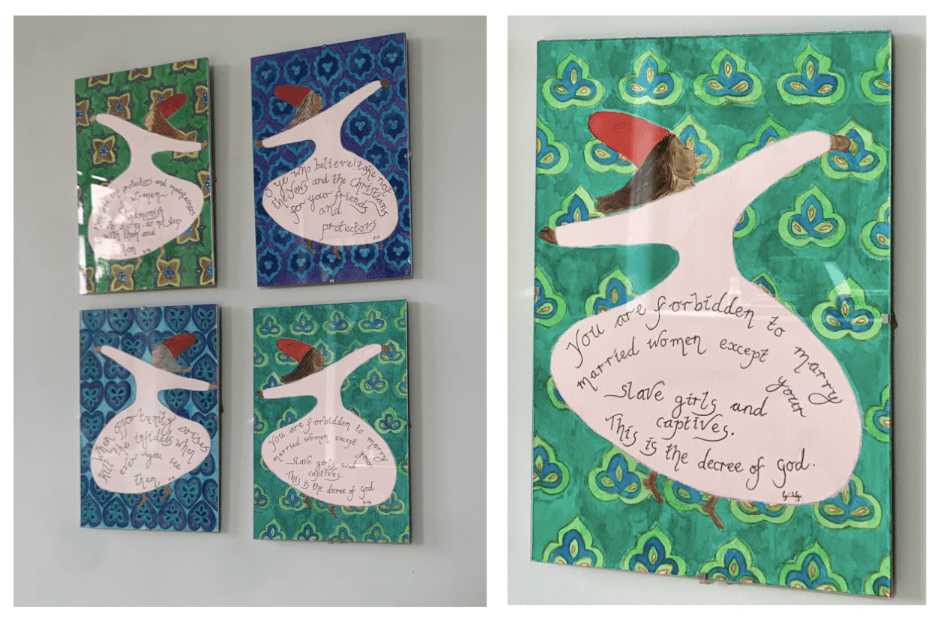
Shabbana
Shabbana’s whirling dervish and Islamic tile inspired pieces juxtapose the beauty of art and mysticism with stark and dour verses from the Koran.“As an ex-Muslim and feminist it was an honour to display at the Women Create event.” Shabanna told me, afterwards. “This was an international yet grassroots event that was uplifting and full of joy, even though the subject matter at times was grim. Victoria did an amazing job of pulling it together, bringing dissident and cancelled artists together in one place, even though sabotage was taking place through subversive methods. But still we rose!”
The third panel
Cancelled Female Creatives in Publishing
Khadija Khan (A Further Inquiry), Victoria Gugenheim (Chair), Jenny Lindsay (Hounded), Jane Clare Jones (Radical Notion), Esmeé Streichailt (Medusa Rising)
Jane Clare Jones
After finishing her PhD, Jane realised that her planned career in academia would necessitate keeping her mouth shut.
“There was no space for academic feminist writing, because pretty much everyone who thought women were female got kicked out of the universities in the 90s and the 2010s.”
After some time of uncertainity, she told us, she cancelled herself by “shouting my mouth off” on Twitter in 2018. This made the decision for her. It was the context in which she found herself unable to follow the career path she had planned, and led to her founding the Radical Notion with Esmé. They wanted to create a space where women could do the thinking that they could no longer do in universities.
Feminism only became established within ‘the Academy’ in the late seventies, and by the end of the 80s it had been eradicated, ‘and with it the entire structure of sex-based analysis’. Women who want to succeed within the university now needed to adhere to the type of feminism that gets male approal.
It is unsurprising that men reward women for ‘destroying the strength of feminist analysis’, and one of the results of this is that women lose funding. It’s not so much that ‘the men’ consciously sabotage women, more that “the funding structures, what we get rewarded for, and what we get promoted for, are not the things that make men feel uncomfortable or nervous.”
There is a lesson to be learned about what happens when feminist spaces get folded into mainstream patriarchal institutions. Being able to understand the patriarchal systems of oppression can save women’s lives, so spaces are needed where vigorous feminist analysis of these systems can take place.
Esmeé Streachailt
Esmée joined us by livestream. She sais she had been thinking recently about the importance of ‘embracing our insurgency’ and wanted to look at cancellation from a historical context, starting with the ‘demotion and murder of the ancient goddesses and the great Mother’. These were extreme forms of cancellation and cultural erasure but are not so far removed from what is being done to women in the current climate.
We see the same impulses at work now as in the 19th century, when women had to publish under male names or initials. She pointed out that the first anthology of women’s poetry, ‘No More Masks!’ edited by Florence Howe and Ellen Bass, was not published until as late as 1972. Much of the history of how women came to occupy the spaces we do, has been lost.
The Women’s Studies department at University of Kansas was founded after 30 women who became known as the ‘February Sisters’ barricaded themselves into a campus building, refusing to come out until the university complied with their demands. Within 30 hours, their demands- for an autonomous women’s studies department, free day care, a sexual health clinic, the ending of sexist wage policies and the recruitment of young women within the faculty- were met.
Importantly, Streachailt said, we need to acknowledge that these women were almost certainly refused more than once before they won. Women have to go to great lengths to have our needs and wants met. Women, when we go through proper channels,are usually told ‘no’, “and end up having to occupy- or chain ourselves to- a building”. Women are no strangers to cancellation, exclusion and rejection, often within the arts and often at the hands of other women. She used the example of French feminist Margurite Stern who was excluded from the ‘collage against femicide’ movement that she herself had started.
“We are insurgents, we should prepare ourselves and each other and the next generation… it creates a cognitive dissonance to have been carving our own humans space into men’s worlds for so many generations, and still be perceived as dangerous strangers.”
She concluded by emphasising the importance of preparing the next generation of young women for the fact that they must continue the fight.
“To be resisted, to be refused, to be hounded; to be silenced, to expect cancellation and to build resilience… we are too far from the end of male dominance to leave our daughters and cousins unprepared for cancellation. Even by the women around them.”
Jenny Lindsay
Jenny joined us by livestream. She always knew she wanted to write and perform, and by 2019, in her ‘old life’, she had established herself as an international performance poet, a programmer of events and a writer of short plays. She had mentored hundreds of teenage school children, won awards, and was able to support herself as a freelancer through hard work and determination.
“A lucky little squirrel indeed,” she observed, describing herself as,”neither entitled, nor ungrateful for the life I had. I knew the privilege of it. The freedom of it.”
In the Scottish literary world, a climate had developed where dissent from gender ideology’s ‘mandatory set of beliefs’ should never be expressed, “whatever regression is being pushed that muzzles women and destroys their rights.”
Being labelled a ‘TERF’ changed Jenny’s life ‘rapidly and irreversibly’. The hardest part for her, she says, is that her cancellation had nothing to do with her talents or abilities. The last job she lost was with a poetry competition run in schools, which she had been involved with for many years. Originally the organisers stood by her, but recently the director confirmed that her writing about gender made her, ‘an unviable poetry educator”.
“Unlike some, I didn’t lose everything overnight – apart from my sanity.”
Would her cancellation have been easier if it had happened all at once, she wondered? She had hoped that lockdown would dampen it, but even friends and colleagues who claimed to support her were not willing to do so openly. One poetry organisation in Scotland has removed all recordings of her performances from their YouTube channel.
She had initially felt no desire to address gender in her art, but decided her only recourse was to write about what happened to her. This resulted in her book, Hounded.
Lindsay has seen her work, “stamped out, as so much is, by the fierce demands of male entitlement to centre their desires, and demand everyone go along with their perception of reality, no matter the cost.”
Yet, she acknowledges, women continue to create, “however we can, in our chosen art forms, with our talents, tenacity, and hard work, in the face of the most extreme hostility many of us have ever known.”
Khadija Khan
Khadija began by saying that as an ex-Muslim and an opinionated woman, her very existence is considered to be blasphemous. Her life has been affected by pressure to conform to religious ideals, societal expectations and gender stereotypes.
“Growing up as a Muslim woman I rarely reflected on why women have been silenced in public spaces for generations. Instead, I absorbed the pervasive misogyny that surrounded me.’
Today she seeks to amplify the voices of countless women born into a culture where they are marginalised from the moment they’re born and face persecution, or even death, for violating family or religious ‘honour’.
“Mothers find themselves forced to silence their daughters, desperate to shield them from the dangerous fallout of challenging traditional gender roles and oppressive societal norms designed by men.”
The misogyny that stems from religious discourse is rarely acknowledged as a form of misogyny. People find it very hard to challenge the ‘divine word’ because they don’t want to cause offence. As a young girl growing up in a conservative Muslim family, raised to believe that women were ‘the very embodiment of original sin’, Kadija quickly learned that her ‘every physical feature was subject to scrutiny in the name of religious morality’.
“I found myself trapped in a cycle of policing my own body… failure to comply risked being labelled a whore merely for wanting to express myself. “
On the subject of women being cancelled in publishing, she says, “I feel like every movement of a woman when she expresses herself is akin to publishing her views, and her thoughts, her vision of how she sees or perceives the society.”
Muslim women who want to express themselves through writing face many obstacles, not just in Muslim majority countries, but here in the UK and often from ‘well-meaning liberal women’. Kadija still faces expectations that she should self-censor in order not to appear ‘anti-Muslim’. Sometimes her editors send her writing back with things changed here and there. “Trying not to appear so harsh on Islam. As if women’s rights were of lesser importance than the religious beliefs themselves.”
Silence is a bottomless pit,” she concluded. “We cannot allow for you to drown out the conversation that needs to happen now. It’s time to break the silence.”
Kelly Frost
Puppet-maker Kelly Frost‘s pieces come to life like magic. This exhibition featured her three-generational hand-carved puppets: so lifelike and with such personality! Kelly’s work on display also featured a series of collages featuring Victorian photographs, and ‘assemblage’ minatures with attention to fine detail.
I asked Kelly to “give me a quote” and she got back to me with this reply, longer than I anticipated but just too perfect to précis, so here it is in full.
“When Claudia asked me to exhibit, I immediately felt that horrid imposter syndrome. Why me? I’m not a proper artist! Surely my work doesn’t belong next to Claudia’s exquisite pots and Con-She’s beautiful and sobering breast binders! But these feelings melted away on installation day. For me personally it was great to feel a sense of pride and surge of confidence in my work when I saw it hanging in the space. “I do belong here,” I thought.
I exhibited three carved wooden puppets. Previously they were laying unceremoniously in a box in my studio, where I would regularly look at them and tell myself ‘I’ll finish them this summer’, ‘I’ll finish them over Xmas’, ‘I’ll finish them before June’….. and on and on it goes.
Knowing they were going to be hanging in an exhibition gave me the kick up the bum I needed. Procrastination is something I struggle with. It’s fear, it’s paralysing perfectionism.
But in May, with a deadline looming, I suddenly sprang into action, refining their heads and making the wigs. Joan has around 80 holes in her head, each one plugged with curly raw sheep’s wool. Each plug must be carefully separated from the bundle of fibres and tied at the base before being pushed into the hole and glued. It’s a labour of love.
I also exhibited two assemblages: La Musique and Fabled Shore, named after the vintage hardback books that make up part of the base. On top of these are open books which form a sort of stage, a set. A collection of tiny objects are arranged on the stage and arranged in a way that plays with scale. A tiny Eiffel Tower sits on top of a wooden dolls’ house chair, next to goldfish in a bag.
Why? I don’t know! It just makes me happy to make them. They are whimsical and fun to look at as well as to make. Almost all the objects were found in charity shops, junk markets and in one of those drawers that we all have in our house. The drawer in which you keep stuff that doesn’t belong anywhere else, where a tiny pencil from a Xmas cracker nestles next to a gaudy, sparkly clip-on earring. We all know that you will only find the second earring once you throw out the first!
I guess you could say Fabled Shore and La Musique are little worlds containing lost and odd objects. Giving these objects a new purpose. I guess that purpose is to make the audience wonder and smile.
For two days I looked at inspiring art and listened to cancelled artists during their talks and the panels. But it wasn’t only that (and that would be enough) it was all the conversations outside with the naughty smokers, the vapers, the wine drinkers and the sun worshippers.
We talked about art, our cancellations, how vulnerable we feel working in the arts, where you can lose your studio for making art that grieves for the kidnapped and murdered Israelis. I chatted with women who lost venues because they state that prostitution is rape not sex work; that mutilating young women’s breasts in the pursuit of ‘trans’ is an abomination.
The crimes for which women artists have been cancelled? Expressing their grief and outrage at murder, torture, rape, medical malpractice and exploitation. This really is a ridiculous situation. It’s unforgivable.
I myself am experiencing a cancellation. In what was strange timing, as soon as I was asked to be part of the exhibition, I started to notice that I’m being frozen out. Puppetry is a tiny world with only 3 puppet theatres in the whole country and only two in London.
90% of my work comes from just one theatre. I don’t know what the future holds for me but, since ‘Women Create’ I am feeling a cautious optimism. Yes, I spoke to many women who are experiencing a cancellation, some catastrophic and overnight, some as a slow creep, but our spirit is not broken. We are down but not out.”
Haram Doodles
Something that is ‘haram’ is forbidden by Islamic law.
It was on the ‘Take Action’ table at the end of the hall that I encountered the work of Haram Doodles, postcards scattered on tables throughout the venue. HD is an anonymous artist, an ex-Muslim woman, who creates simple but powerful cartoons surrounding the oppression of women in Islam, and the absurdity of many religious edicts.
I loved her style, and asked her for a few words about her work and the conference. “I’m an ex-Muslim atheist woman who creates art as an act of resistance because my existence is also an act of resistance,” she told me.
“It’s really special when women get together and share, and have spaces to belong and come together in solidarity. So we can really talk about the things that generally society sees as blasphemous, or as shameful. Especially when it comes to women and women’s bodies. So it’s just really special to be here and be part of what truly is a celebration of women.”
‘Haram’ was also the first speaker on the next panel.
The fourth panel
Revolution Needs Culture- We are that Culture!
Con-She, Haram Doodles, Claudia Clare, Victoria Gugenheim (Chair)
Haram Doodles
As a little girl, she was told that if she didn’t stop drawing, Allah would make her breathe life into all of her drawings after she died, as a punishment. She was so frightened by this idea, that she stopped drawing ‘for years and years’ not doodling again until she was an adult.
As a child growing up in America, she endured taunts at school for ‘being the only brown kid’, She says such behaviour would be better described as ‘anti-Muslim hate’ than Islamophobia, as it better captures the prejudice faced by Muslims.
“Three years ago, I started Haram Doodles, not knowing where it was going to go, or how people were going to see them, but I really wanted to create content that spoke to me, and that I wish I’d had on my own journey out of Islam.”
Her style is deliberately child-like, as she says,‘a lot can be said with a simple drawing’. Her 10,000 Instagram followers are not only ex-Muslims, but ex-Christians, ex-Mormons and ex-Jews. Many have reached out and shared that they were afraid of leaving their religion and that her doodles “provided some space for belonging and affirmation”.
That contact was enough for her to know she had to continue, despite the fact that apostasy and blasphemy are punishable by death in Islam. She acknowledges that to continue drawing is potentially an ongoing danger to her safety “and that is a risk I shall continue to take.”.
She thinks it is sad that her own family can’t see ‘life outside Islam’, but is clear that she doesn’t hate them for it, as she believes it’s important to separate the ideology from the people indoctrinated by the ideology, “just like I was”.
Some religious people do try to convert her, or bombard her with religious texts, but she ignores them so she can focus on what matters to her.
“I ignore all Muslims, I ignore all the religious folks because I’m not there for them. I’m there for ex-Muslims.”
Claudia Clare
“I’m of the opinion that we have been having something of a cultural revolution recently- a reassertion of the male’s divine right to our spaces and opportunities. We see this writ large in gender theory and in trans rights activism which seems to be a primarily about destroying women’s rights.”
Claudia says she well remembers that when she was at art school in the 80s there were no female tutors. It was an open secret that many of the female students had been selected more for their potential as lovers for the tutors than on the basis of their artistic talent. Claudia is concerned that the Arts thrall to ‘gender’ may result in a return to these times.
“I think culture has played a major part in galvanising and fixing the rise the lies of gender in the arts. It’s often said over the arts is hopelessly captured. I think it’s not so much captured, I think that it was instrumental in the capturing of everywhere else.”
Claudia notes that this has been going on for some time. Almost twenty years ago, she noticed that 80s iconic lesbian artists Lubaina Himid and Maud Sulter, drivers of the black art movement, were not featured in a ‘lesbian’ exhibition at the V&A. Yet, she recalls that during LGBT History month, organisers rolled out a nail bar for ‘transwomen’.
“That is not part of lesbian and gay history,” she said.
Claudia told us that a feminist writer once challenged her as to how she could intend to work in the art world after graduating, when ‘absolutely central to the nature of art is the naked woman’. This uncomfortable truth is present not just in art, but in how artists models were treated, and the art world’s historic links to the sex industry.
She concluded by saying the visual arts ‘is simultaneously creating and establishing what is normal’ and ‘feminism shuold ignore the visuall arts at its peril.’
Con-She
The next speaker was an anonymous artist from Glasgow, who creates as a performance artist character called Con-She. A play on words, Con-She can mean both ‘with her’ and ‘conscientious objector’. She said she had recently been reflecting on the new movement that women are creating going forward.
“I think that through all the pain and anguish of cancellation, the one thing that can be said about the cultural output that comes from this movement is that it is authentic. And for my money, that’s the most important thing.”
Political art must have some sort of connection to truth, in the broadest sense, Con-She stated. Good art must be authentic and honest, and it can be incredibly powerful for this reason.
“It can tell us about something that’s created from the heart in a moment of great turmoil. And it tells us something about the world, through the lens of a single human being’s authentic response to it. And that’s what art should do.”
This, she says, is the opposite of the current situation in the mainstream art world, where the current approach is to encourage us to only identify with ‘people who are like us in the most superficial ways’. The visual arts especially is engaged in what Con-She calls the game of ‘Spartacus Oppression’, a grotesque appropriation of actual oppression. She views the current mainstream purpose of art as little more than a tool to ‘express the narcissistic concerns of the middle classes,’ describing it as, “a kind of weird pantomime of middle-class people, pretending to be oppressed because they’ve dyed their hair blue to compete for intersectional traction.”
The result is that our movement is currently both a genuine battle and a counterculture. Thus, “we find ourselves necessarily in the space of authenticity (which) makes our work inherently stronger.”
But the movement is not yet mature, for all its brilliant and passionate activism, she concludes. While imagery and music are unparallelled their effectiveness at bringing people together, we need to support ‘more contemplative and nuanced’ work as well, in order to reach a position where we have grown into ‘a fully-fledged art movement, rather than a political movement with imagery’.
There was a Q&A after the session.
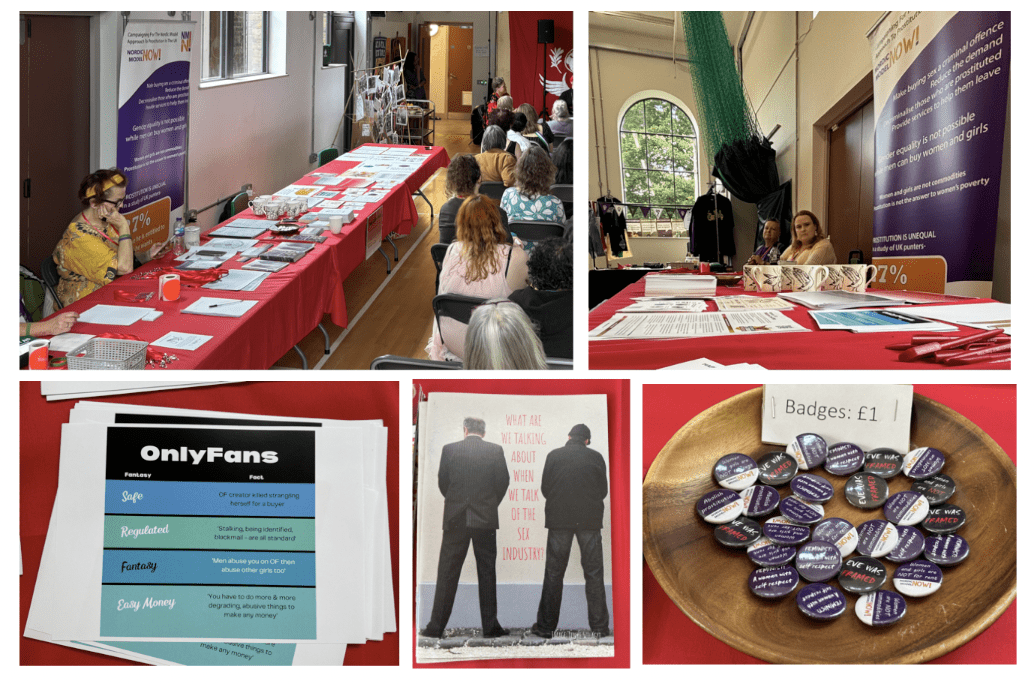
Nordic Model Now
Nordic Model Now is a group concerned with prostitution, who advocate for the ‘nordic model’ approach, which, very simply put, helps women who want to leave the industry, and prosecutes the men who use them. Established in 2016, it campaigns for the abolition of prostitution and related practices.Nordic Model Now gives a voice to prostituted women and provides excellent resources, many of them from a first-hand perspective, explaining the damage done by the sex industry. It’s no exaggeration to say their website is one of the most accessible and informative around, and I was delighted to be able to acquire a couple of copies of their booklet ‘What are we talking about when we talk of the sex industry?’. You can purchase the booklet on their website, or download a free copy here.
Everything else
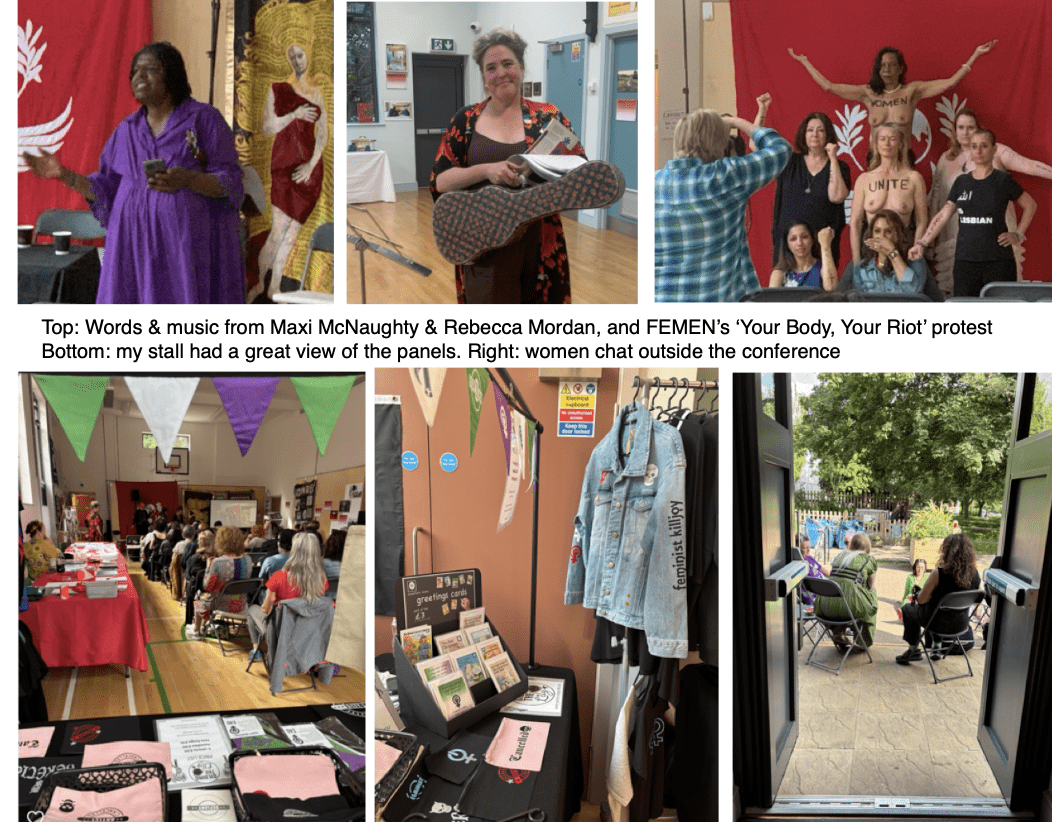
There was so much else! There was more music, poetry recitals, perfomances and a topless bodyart protest, “in solidarity with with cancelled women, creatives and female artists around the world at risk- including women at risk for dancing in the street.”
I left long before the cxonference wound up for the evening. What an amazing day!
I originally thought my write-up would take me a few days to complete. Instead it’s taken the best part of two weeks; there was so much to cover and I was loathe to leave anything out.
There were things I overlooked, right under my eyes, or suspended above my head. Below left, for example, I’ve captured a piece I didn’t notice at the time: the textile hanging, stitched by Russian exiles Maria and Polina Pomidor, ‘Search for the Baltic Way’. The piece was made for the Women Create exhibition and remembers the extraordinary human chain of 2 million people, formed in 1989, stretching 690 kilometres across Lithuania, Latvia and Estonia, in protest against the Soviet occupation.
While I’ve inevitably left so much out, I hope I’ve managed to give some idea of what an incredible day it was.
“Women create, and by God, do we not create the ultimate? We’re the best creators this world has ever seen. The best in this whole world! And this venue, and this event is so essential. To keep us built up and moving forward. Women Create is necessary; it’s needed, and our own spaces are needed and our own groups are needed- because women together, we can move mountains. And I believe every word of that.”
Julie M, ‘Women Won’t Wheesht’
I’ll finish up with a short interview with founder and creator Victoria Gugenheim.
Making ‘Women Create’ happen
Victoria Gugenheim is a world reknowned body artist, no stranger to controversy, and midwife to the ‘Women Create’ conference. She is already planning her next event, in Scotland, and other international events under the ‘Women Create’ banner.
“This whole thing has been a real struggle and a labour of love. I knew it needed to happen because there are so many women being cancelled and censored and silenced, and we needed a place to come together that was specifically for female artists…”
Victoria told me that she had approached forty organisations in the hunt for funding, and around three hundred venues. She was frequently rejected with claims such as “it’s not really in our remit,” or told “your event doesn’t align with our inclusion policy”.
After finally securing the venue the booking was cancelled by the centre manger, who told her, “some of your artists are transphobic so you can’t use this space’. Gugenheim then approached Maya Forstater for help in securing the venue.
I asked how they had eventually funded the event.
“All of the materials I paid for myself,” Victoria told me. “The venue, everything! I had to pull heaven and earth to make this happen!”
Victoria said that she felt that traditional feminist conferences could leave women feeling despairing. “You need art to uplift!” she said. “To question things and shake things up… because if you don’t have that you will lose the fight, because your human spirit is going to be so kowtowed because of all the horror and the pain and suffering that is going on in the world. Joy is a feminist issue- at what price is your liberation if all you’re doing is being miserable about the state of the world all the time?”
I couldn’t be prouder of the women we’ve got here. I think for the first time in history we’ve got ‘boots on the ground’ women’s rights activists exhibiting in the same exhibition as V&A artists and Tate Modern artists.
That’s what Women Create is about, and that’s why it needs to happen. From here all I want to do is grow it, add more artists; take it around the world and see the strength of these women in action!”
Here, you can read more about the individual artists who exhibited at the 2025 conference.
Here, you can see the program of events.

 The ‘Women Create’ conference was the brainchild of
The ‘Women Create’ conference was the brainchild of 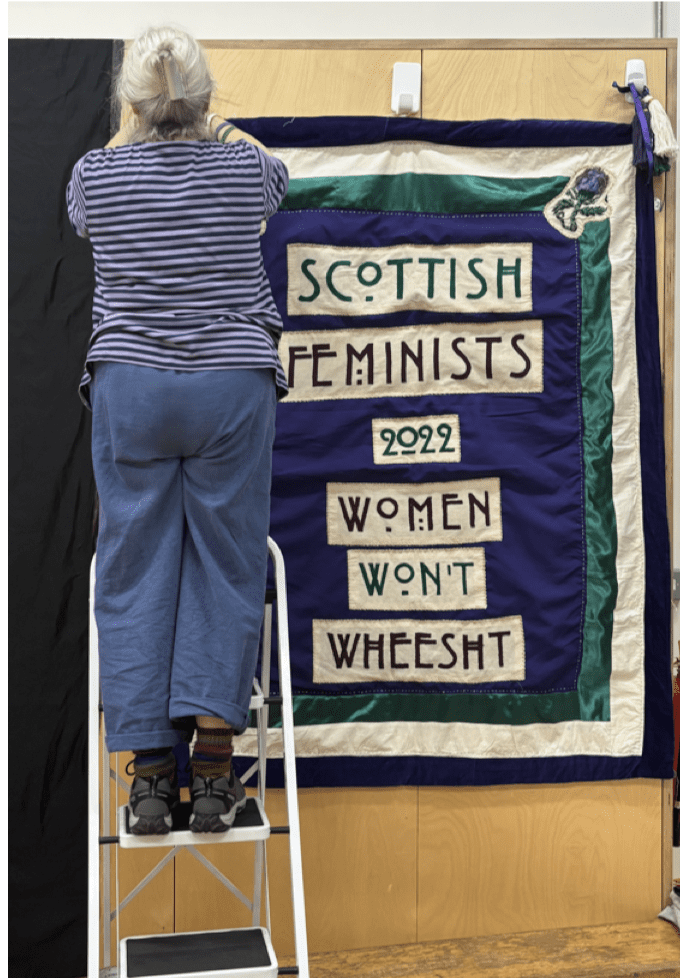 We had been allocated several hours on the Thursday evening to set everything up, and things were predictably chaotic. One of the more Sisyphean tasks was trying to attach dark curtains and posters to the large arched windows of the main hall. Some of the panels were using projectors, and a film, Vaishnavi Sundar’s ‘
We had been allocated several hours on the Thursday evening to set everything up, and things were predictably chaotic. One of the more Sisyphean tasks was trying to attach dark curtains and posters to the large arched windows of the main hall. Some of the panels were using projectors, and a film, Vaishnavi Sundar’s ‘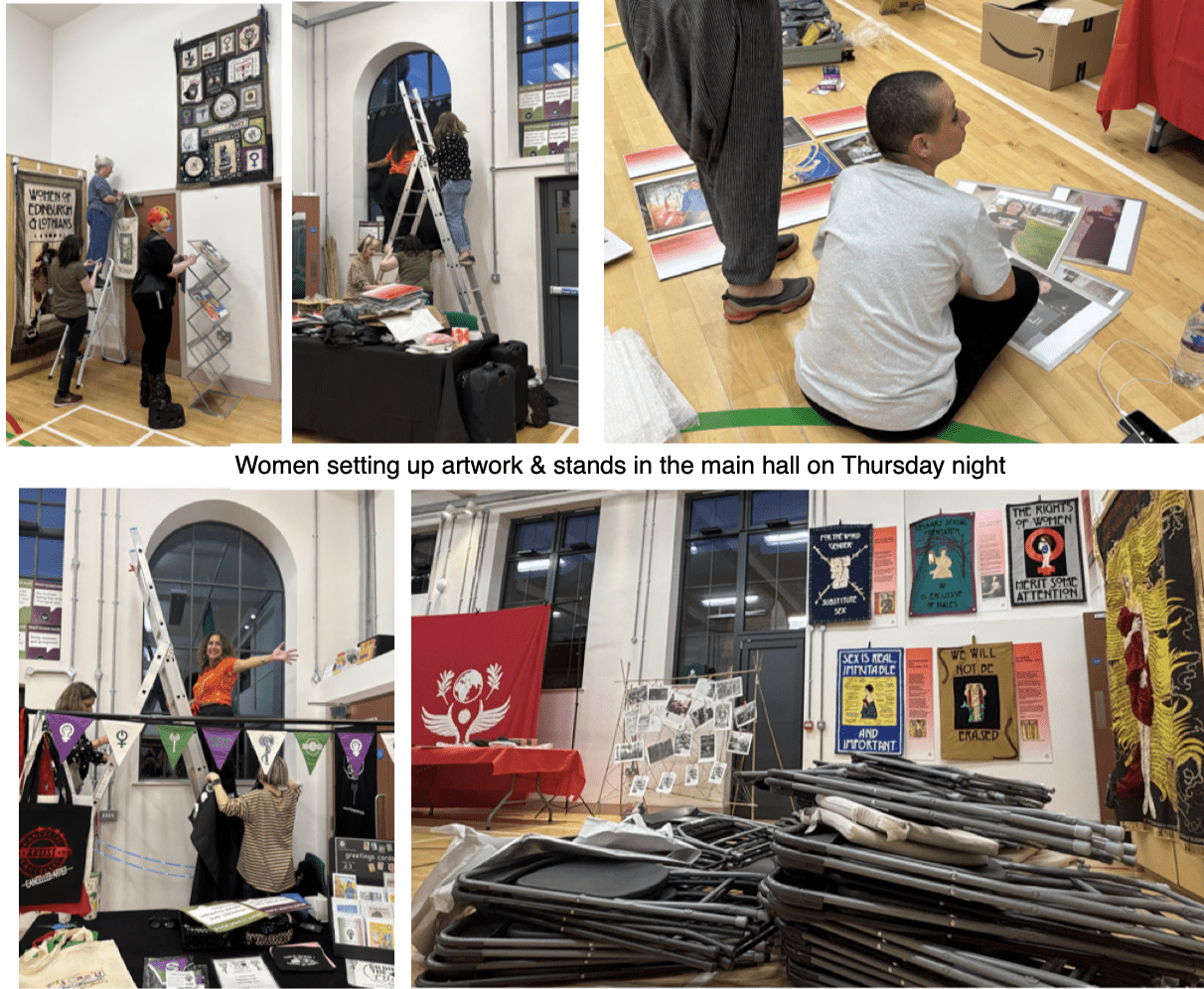 You can view the full program for ‘Women Create’
You can view the full program for ‘Women Create’  The next morning we were back at the venue bright and early. It was a hot sunny day, and when I arrived at 9.30, the stewards were already set up outside in a splash of purple colour. At ten o’clock, attendees began to arrive for registration. It was a relief to have done all my unpacking and arranging the night before and to just sidle into place with a flask of coffee and watch things unfold around me.
The next morning we were back at the venue bright and early. It was a hot sunny day, and when I arrived at 9.30, the stewards were already set up outside in a splash of purple colour. At ten o’clock, attendees began to arrive for registration. It was a relief to have done all my unpacking and arranging the night before and to just sidle into place with a flask of coffee and watch things unfold around me. These really have to be seen to be appreciated. Created with a mixture embroidery, appliquéand felting, often featuring intricate details that need to be viewed with the naked eye.
These really have to be seen to be appreciated. Created with a mixture embroidery, appliquéand felting, often featuring intricate details that need to be viewed with the naked eye. 
 I checked out the stands next to my stall and watched the gathering women as they chose seats and prepared for the first panel.
I checked out the stands next to my stall and watched the gathering women as they chose seats and prepared for the first panel. 
 Ray observed that she had no powerpoint or notes, but she did have a lot to say. Greenham has been erased from feminist history, she told us, but she and others have been able to undo this omission.
Ray observed that she had no powerpoint or notes, but she did have a lot to say. Greenham has been erased from feminist history, she told us, but she and others have been able to undo this omission.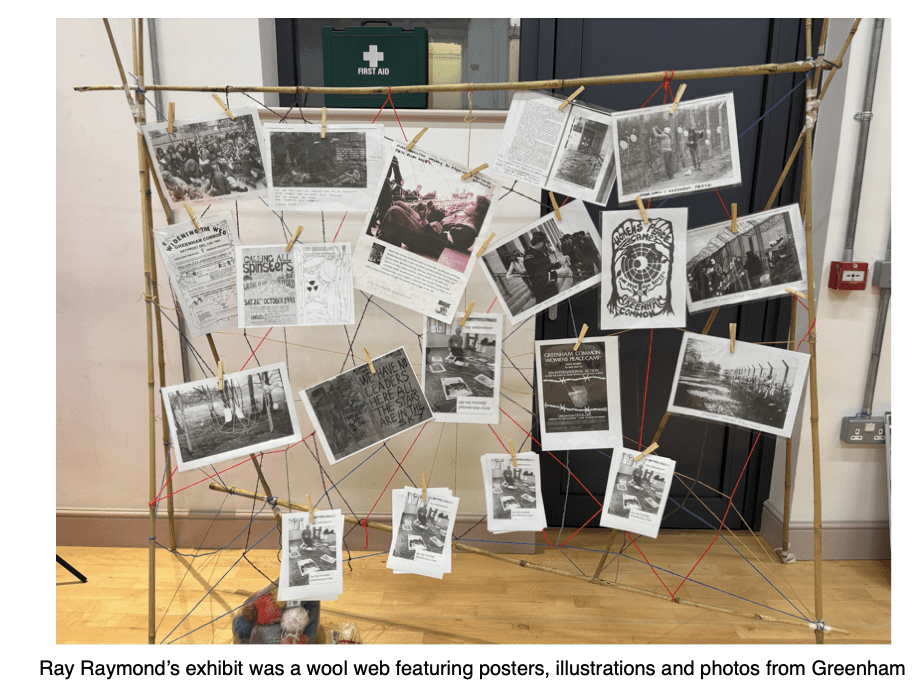
 The next speaker, Betty Lachgar, began by telling us that her T-shirt read ‘Allah is a lesbian’. After wearing it at a conference in Germany in 2020, she was arrested on her return to Morocco. The investigation is still in progress.
The next speaker, Betty Lachgar, began by telling us that her T-shirt read ‘Allah is a lesbian’. After wearing it at a conference in Germany in 2020, she was arrested on her return to Morocco. The investigation is still in progress.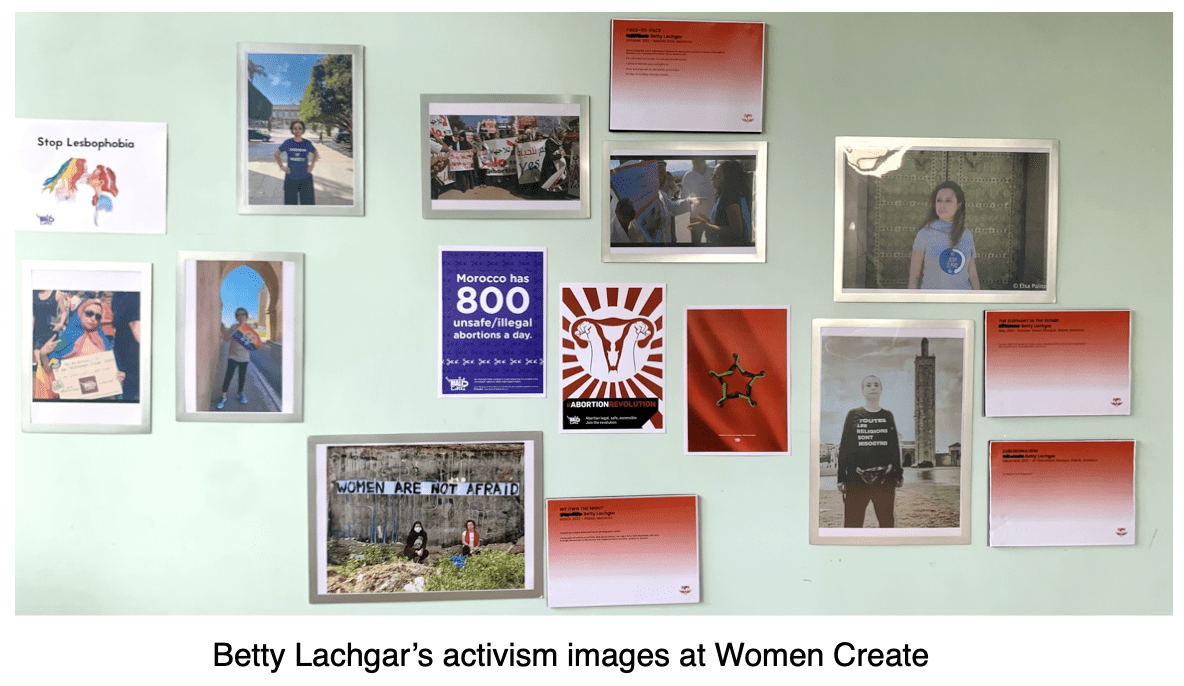

 Her own art consists of photographs or protest and portraits of FEMEN activists, and is seen as highly controversial.
Her own art consists of photographs or protest and portraits of FEMEN activists, and is seen as highly controversial. 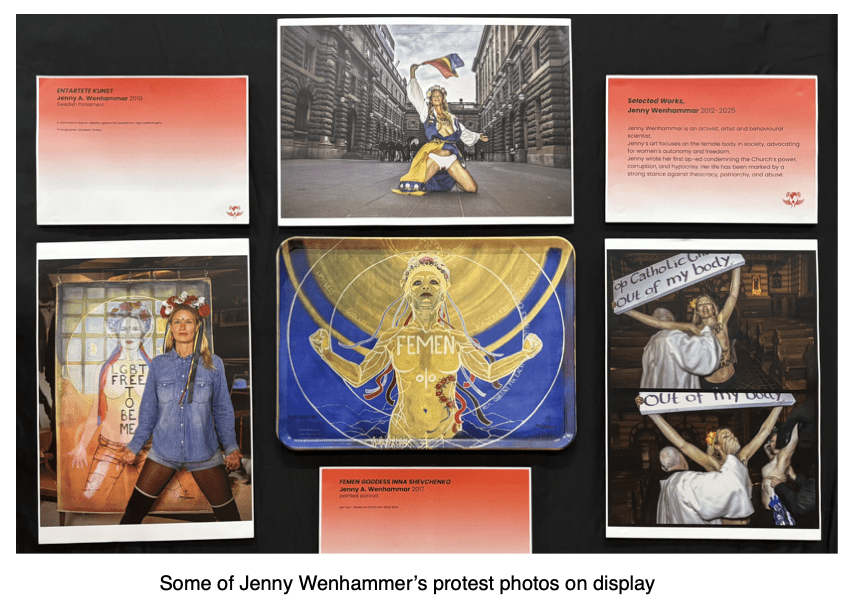

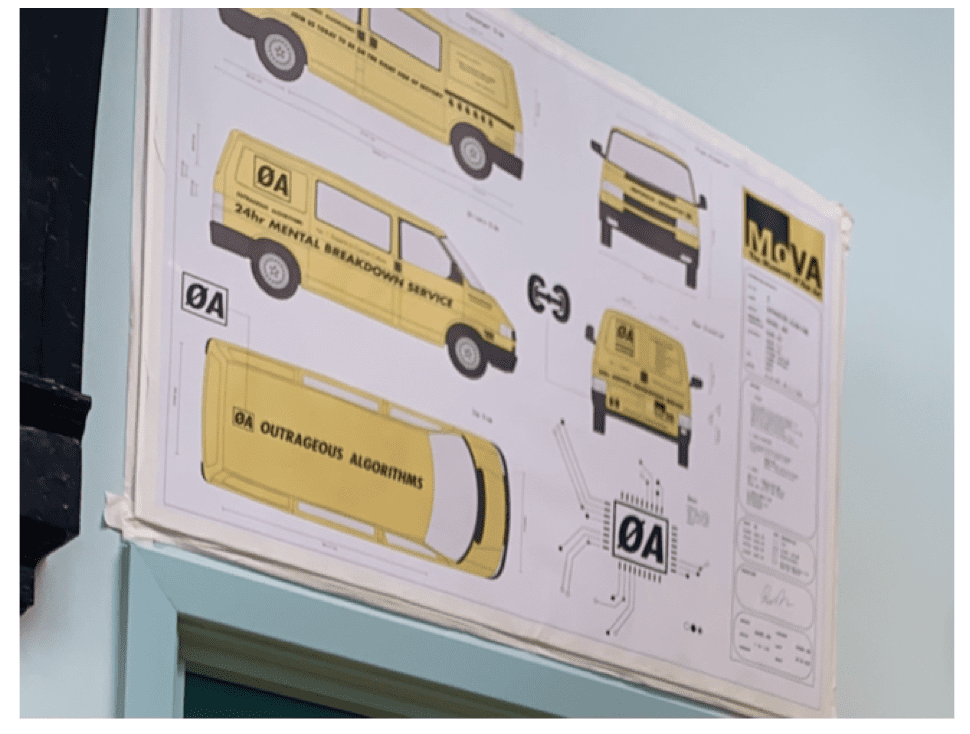 During the COVID lockdowns, Ara turned her van into a mobile art exhibit with ’24 Hour Merntal Breakdown Service’ written along the side. Sightings went viral on social media. You can learn more about Outrageous Algorithms (A fourth emergency service for todays problems)
During the COVID lockdowns, Ara turned her van into a mobile art exhibit with ’24 Hour Merntal Breakdown Service’ written along the side. Sightings went viral on social media. You can learn more about Outrageous Algorithms (A fourth emergency service for todays problems) 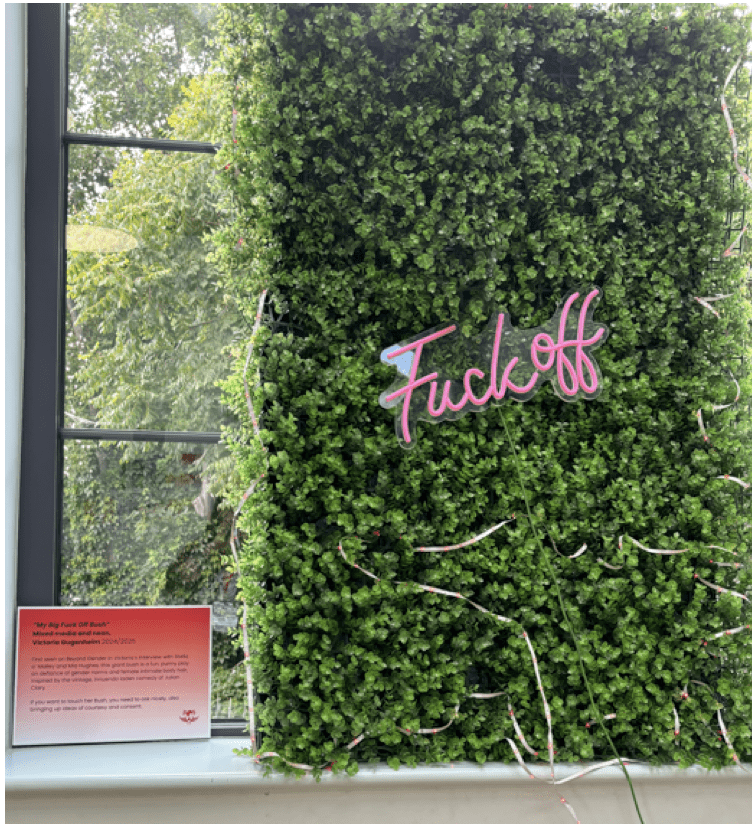







 After finishing her PhD, Jane realised that her planned career in academia would necessitate keeping her mouth shut.
After finishing her PhD, Jane realised that her planned career in academia would necessitate keeping her mouth shut.
 Jenny joined us by livestream. She
Jenny joined us by livestream. She She had initially felt no desire to address gender in her art, but decided her only recourse was to write about what happened to her. This resulted in her book,
She had initially felt no desire to address gender in her art, but decided her only recourse was to write about what happened to her. This resulted in her book, 
 Puppet-maker
Puppet-maker 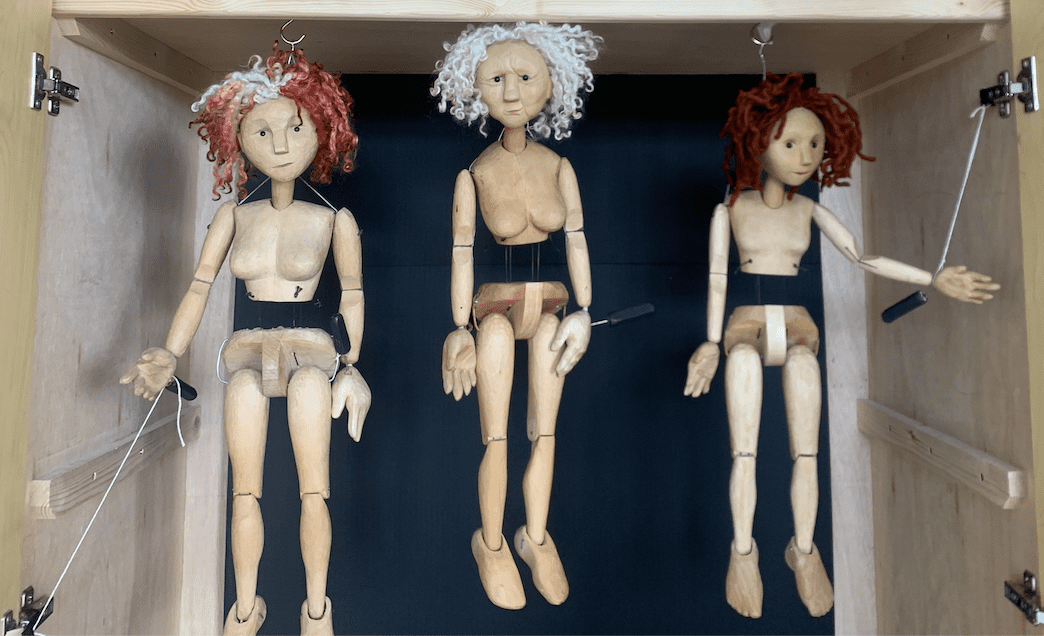
 “When Claudia asked me to exhibit, I immediately felt that horrid imposter syndrome. Why me? I’m not a proper artist! Surely my work doesn’t belong next to Claudia’s exquisite pots and Con-She’s beautiful and sobering breast binders! But these feelings melted away on installation day. For me personally it was great to feel a sense of pride and surge of confidence in my work when I saw it hanging in the space. “I do belong here,” I thought.
“When Claudia asked me to exhibit, I immediately felt that horrid imposter syndrome. Why me? I’m not a proper artist! Surely my work doesn’t belong next to Claudia’s exquisite pots and Con-She’s beautiful and sobering breast binders! But these feelings melted away on installation day. For me personally it was great to feel a sense of pride and surge of confidence in my work when I saw it hanging in the space. “I do belong here,” I thought.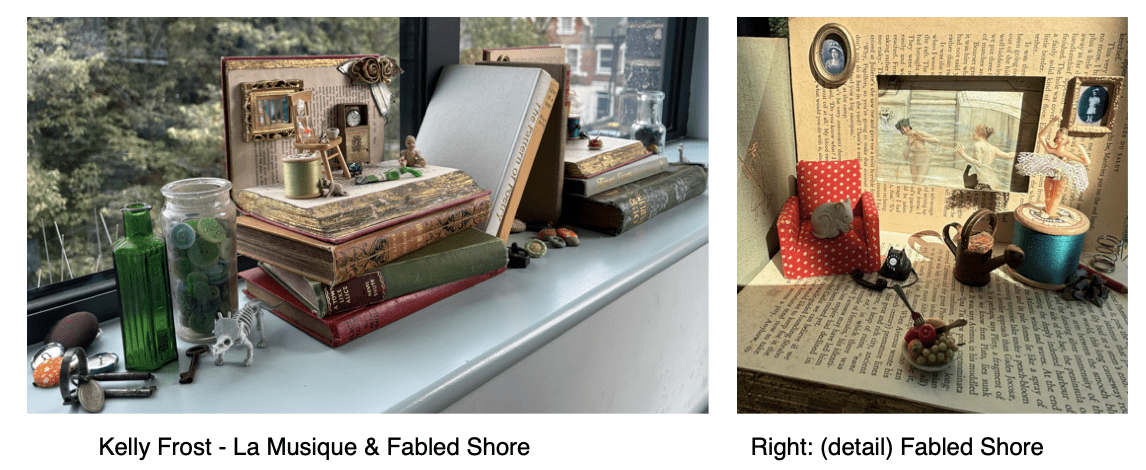
 Why? I don’t know! It just makes me happy to make them. They are whimsical and fun to look at as well as to make. Almost all the objects were found in charity shops, junk markets and in one of those drawers that we all have in our house. The drawer in which you keep stuff that doesn’t belong anywhere else, where a tiny pencil from a Xmas cracker nestles next to a gaudy, sparkly clip-on earring. We all know that you will only find the second earring once you throw out the first!
Why? I don’t know! It just makes me happy to make them. They are whimsical and fun to look at as well as to make. Almost all the objects were found in charity shops, junk markets and in one of those drawers that we all have in our house. The drawer in which you keep stuff that doesn’t belong anywhere else, where a tiny pencil from a Xmas cracker nestles next to a gaudy, sparkly clip-on earring. We all know that you will only find the second earring once you throw out the first!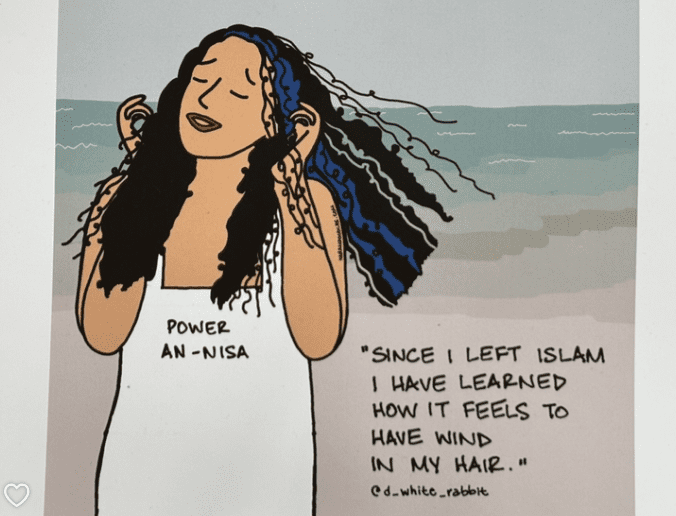 Something that is ‘haram’ is forbidden by Islamic law.
Something that is ‘haram’ is forbidden by Islamic law.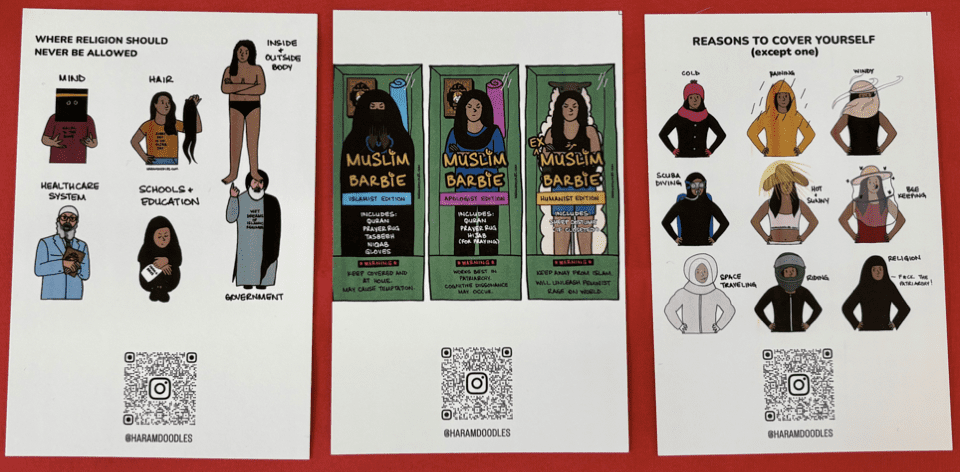 “I’m an ex-Muslim atheist woman who creates art as an act of resistance because my existence is also an act of resistance,” she told me.
“I’m an ex-Muslim atheist woman who creates art as an act of resistance because my existence is also an act of resistance,” she told me. “It’s really special when women get together and share, and have spaces to belong and come together in solidarity. So we can really talk about the things that generally society sees as blasphemous, or as shameful. Especially when it comes to women and women’s bodies. So it’s just really special to be here and be part of what truly is a celebration of women.”
“It’s really special when women get together and share, and have spaces to belong and come together in solidarity. So we can really talk about the things that generally society sees as blasphemous, or as shameful. Especially when it comes to women and women’s bodies. So it’s just really special to be here and be part of what truly is a celebration of women.” As a little girl, she was told that if she didn’t stop drawing, Allah would make her breathe life into all of her drawings after she died, as a punishment. She was so frightened by this idea, that she stopped drawing ‘for years and years’ not doodling again until she was an adult.
As a little girl, she was told that if she didn’t stop drawing, Allah would make her breathe life into all of her drawings after she died, as a punishment. She was so frightened by this idea, that she stopped drawing ‘for years and years’ not doodling again until she was an adult.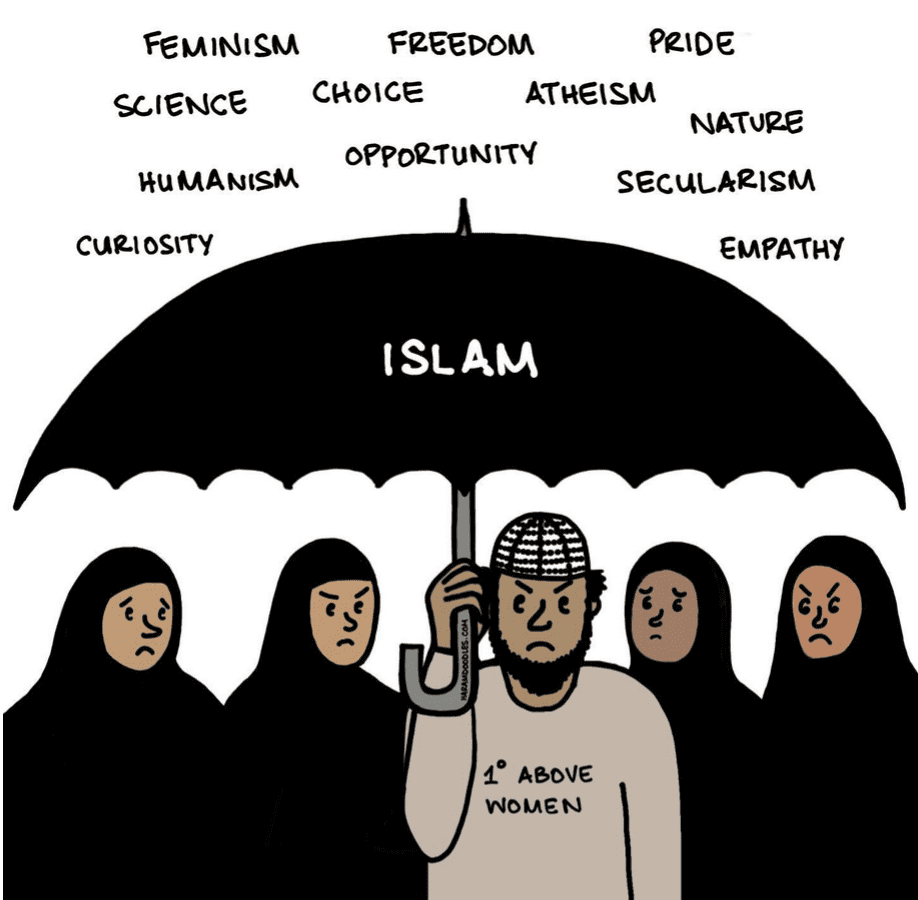 That contact was enough for her to know she had to continue, despite the fact that
That contact was enough for her to know she had to continue, despite the fact that


 Victoria Gugenheim
Victoria Gugenheim

 “Women have spoken; the Supreme Court has spoken, but the fight is not over. If anybody fancies a Bank Holiday Monday down at the Men’s Pond, I’ll be there next Monday. The Men’s Pond, because they’re still saying, ‘we’ll think about it’. Fuck that. The Supreme Court has spoken. We’re taking back our spaces and we’re proving it now.”
“Women have spoken; the Supreme Court has spoken, but the fight is not over. If anybody fancies a Bank Holiday Monday down at the Men’s Pond, I’ll be there next Monday. The Men’s Pond, because they’re still saying, ‘we’ll think about it’. Fuck that. The Supreme Court has spoken. We’re taking back our spaces and we’re proving it now.” Initially, news of the protest was spread by mo
Initially, news of the protest was spread by mo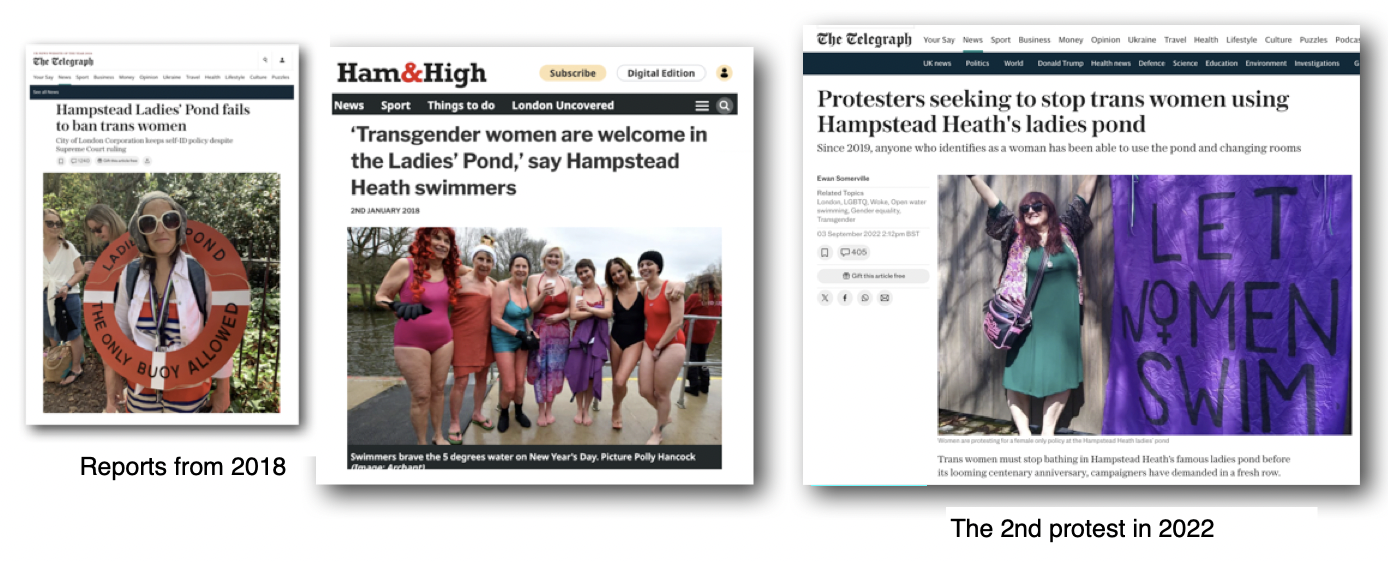



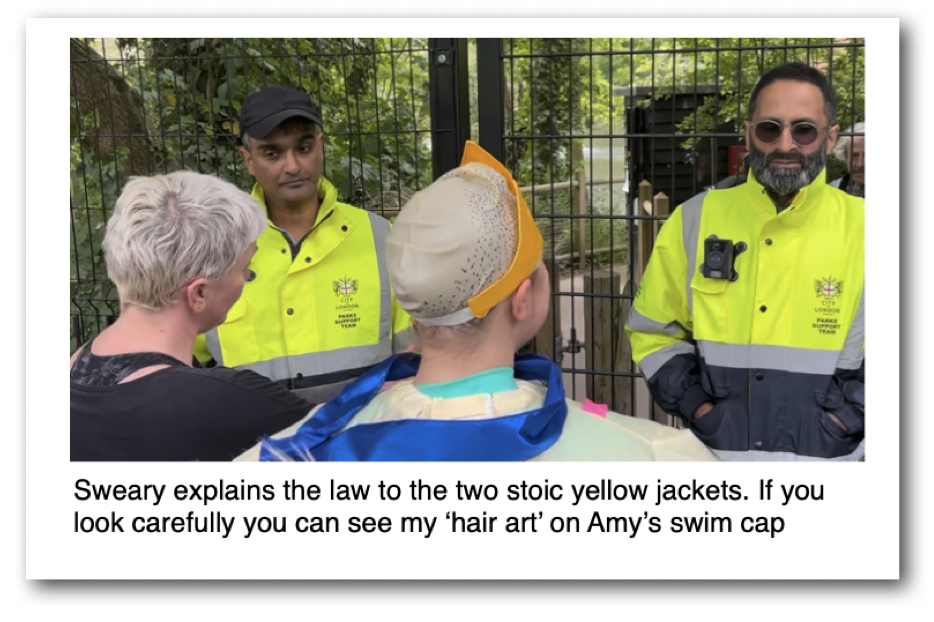
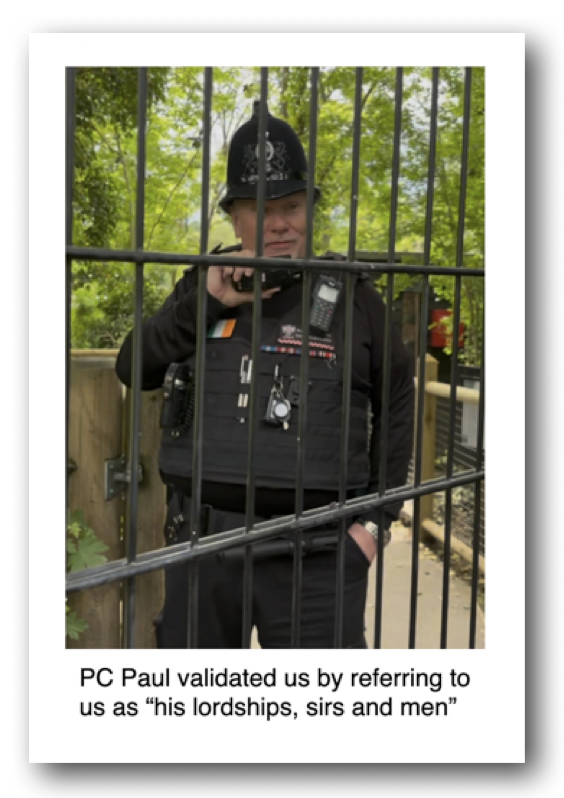
 I looked round at our little posse of manly men and found it hard to disagree with PC Paul. Flags, banners, placards and weird costumes- none of this suggested that we were just a group of guys out for a swim. Other members of the group were not so easily led from their goal.
I looked round at our little posse of manly men and found it hard to disagree with PC Paul. Flags, banners, placards and weird costumes- none of this suggested that we were just a group of guys out for a swim. Other members of the group were not so easily led from their goal.
 When I heard the cry of “
When I heard the cry of “
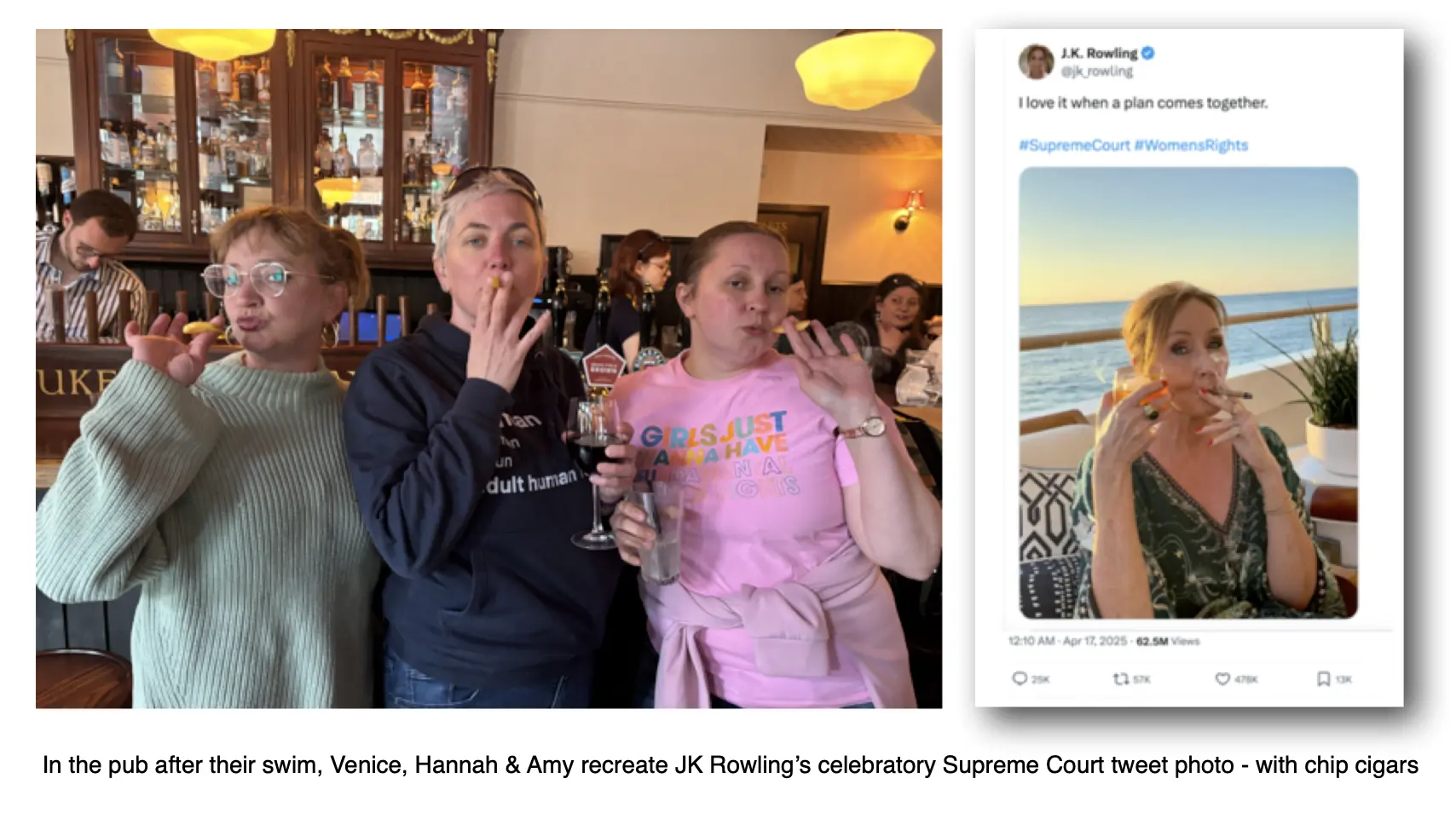
 In all, five of the women broke free from our little band of merry men and took the plunge. Bedraggled but triumphant, they swan for about 15 or 20 minutes. Draped in towels and coats and whatever else they had to hand, they shivered and dried themselves off, mission accomplished, and we headed off to the pub and then later to the park.
In all, five of the women broke free from our little band of merry men and took the plunge. Bedraggled but triumphant, they swan for about 15 or 20 minutes. Draped in towels and coats and whatever else they had to hand, they shivered and dried themselves off, mission accomplished, and we headed off to the pub and then later to the park.
 “When I saw the video of Amy speaking at LWS, calling us to action at the ponds again, I just knew I had to be there too. She is the brilliant, ridiculous genius that came up with Man Friday back in 2018 – I was only ever riding her coattails.
“When I saw the video of Amy speaking at LWS, calling us to action at the ponds again, I just knew I had to be there too. She is the brilliant, ridiculous genius that came up with Man Friday back in 2018 – I was only ever riding her coattails.

 “At the women’s pond, it’s not just about getting undressed with privacy, it’s about spending time together in the meadow away from the male gaze. This is really important for all women but it becomes more important for lesbians, for orthodox Jewish women, for Muslim women and for any woman who feels uneasy or frightened in front of men.
“At the women’s pond, it’s not just about getting undressed with privacy, it’s about spending time together in the meadow away from the male gaze. This is really important for all women but it becomes more important for lesbians, for orthodox Jewish women, for Muslim women and for any woman who feels uneasy or frightened in front of men. “I thought the best thing about today was that it was a reunion of the original Man Friday team from the action back in 2018. Hannah Clarke – also known as Sweary Godmother- just reappeared after she was summoned by the fabulous Amy Desir! They were the OG men’s pond campaigners and I’m so happy to support them today.
“I thought the best thing about today was that it was a reunion of the original Man Friday team from the action back in 2018. Hannah Clarke – also known as Sweary Godmother- just reappeared after she was summoned by the fabulous Amy Desir! They were the OG men’s pond campaigners and I’m so happy to support them today. 


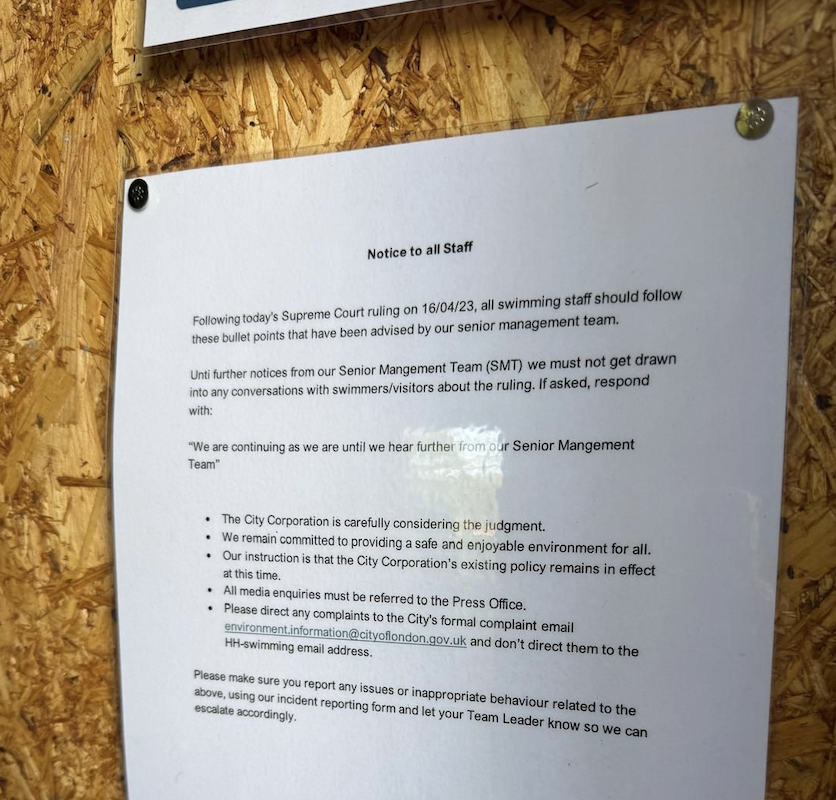 It seems a sign had been spotted on the noticeboard in the staff hut, warning staff not to discuss the Supreme Court ruling or pond policy with swimmers. Staff should report ‘any issues’ and if questioned say only,
It seems a sign had been spotted on the noticeboard in the staff hut, warning staff not to discuss the Supreme Court ruling or pond policy with swimmers. Staff should report ‘any issues’ and if questioned say only,