Why did we need a protest?
Why did we need a protest?
The Supreme Court has changed no laws; it has taken rights away from no-one. It has merely clarified- for those who needed such clarification- that a man is not a woman.
In May 2025, the Supreme Court ruled in favour of For Women Scotland and confirmed that references to ‘sex’, ‘man’ and ‘woman’ in the Equality Act refer to biological sex (a person’s sex at birth). A Gender Recognition Certificate (GRC) does not turn a man into a woman (or vice versa).
For the purposes of the Equality Act, a woman is a biological woman, an ‘actual’ woman. An Adult Human Female. Not A Man. Is not nor-has-ever-been in possession of a penis. And it was ever thus.
That we needed the highest court in the land to tell us what a woman is, is in itself both surreal and absurd. That even after the aforementioned court had spoken, people would claim the ruling was ‘difficult’ or ‘complicated’ shows just what a grip gender ideology has on the collective bollocks of our culture. That the government would drag its feet after such a ruling should be, quite frankly, unbelievable.
Yet those who thought things were going to change after the ruling were bemused to find that very little did. In October, the Equality and Human Rights Commission (EHRC) said its advice based on the Supreme Court ruling had been removed from its website. From councils to youth clubs, groups waffled on about ‘waiting for guidance’ as if they hadn’t just had it spelled out in black and white by the highest court in the land.
But when rapists get put in women’s prisons, & government ministers such as Scotland’s Kirsty Blackman declare theat they’re not really quite sure what sex they are, we know that the woowoo boat has long set sail.
The situation in prisons is a good example of the current climate of evasion and apathy. The public is led to believe that male prisoners are no longer put in women’s prisons. Current policy maintains that men (aka transgender women) will not be placed in women’s prisons – “with exemptions only to be made in the most exceptional cases”. The irony here is that such a situation is already ‘exceptional’ and this little phrase provides a ‘get out of jail free’ clause rendering the rest of the policy virtually meaningless in the wrong hands. And this aside, there are still men in women’s prisons.
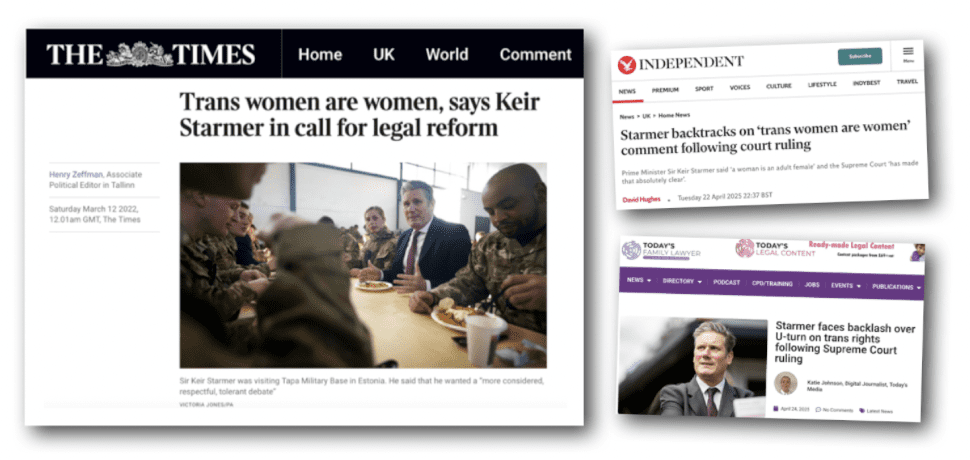
We are living in a country where it makes headlines both when the head of state announces that he thinks a man can become a woman, and again when he announces he’s changed his mind. Starmer now claims to support the Supreme Court ruling but has made little effort to ensure it is implemented.
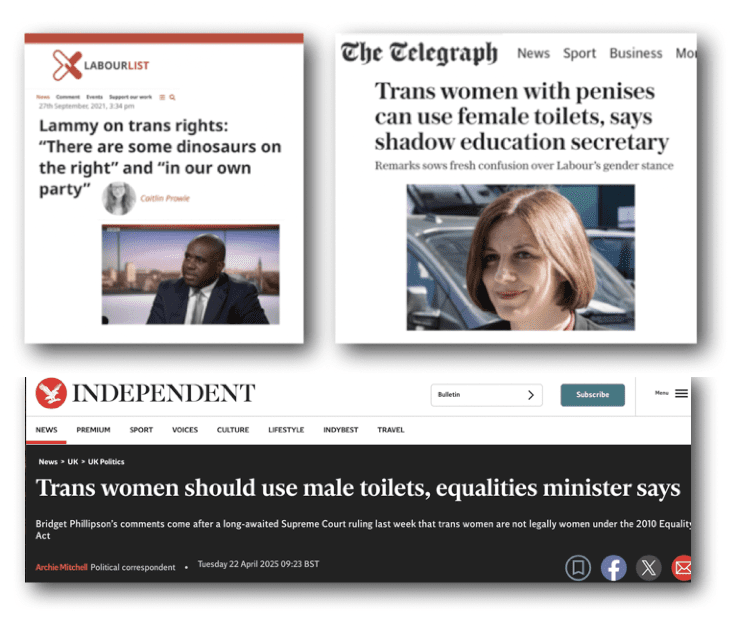
Add into the mix the insipid word salad of Bridget Philipson (now Secretary of State for Education and Minister for Women and Equalities) and the astonishing ignorance of David Lammy (now Deputy Prime Minister, Lord Chancellor, and Secretary of State for Justice), and you start to see what we are up against.
In 2024 Philipson said someone who had gone through ‘quite an extensive process’ to ‘change gender’ should be allowed to use the toilets of their ‘aquired gender’. After the Supreme Court ruling in April, she changed her tune. Nothing has actually been done, however.
Compared to David Lammy, who seems to believe that men can magically grow a cervix, Philipson is a beacon of rational thought.
“It’s probably the case that trans women don’t have ovaries- but a cervix, I understand, is something you can have following various procedures and hormone treatments.” mused Lammy.
In 2021 Lammy referred to sex realists as ‘dinosaurs on the right… and in our own party’ and accused women of wanting to ‘hoard (their) rights’.
Fast forward several years and little seems to have changed. Lammy has stopped with the absurd comments, but nothing more rational has taken their place. A ‘real mess’ indeed, as recognised even by the Grauniad.
Time to Organise
It was in this post-Supreme-Court-ruling climate, that a small group of women from all over England began discussing how they might organise something the government would have to notice; something to shame our politicians and let them know we are watching. The government needed to be held to account- at very least it needed a bloody good telling off. A seed of action began to sprout.
“We’re just a bunch of ordinary, dedicated women,” one of the organisers told me. “We were really angry that nothing had been done since the Supreme Court judgement. No government departments had enacted anything, or brought anything forward, changed policies or even removed old policies.
The whole event was organised over WhatsApp and Zoom, on a shoestring, from our own contacts and within our own networks.”
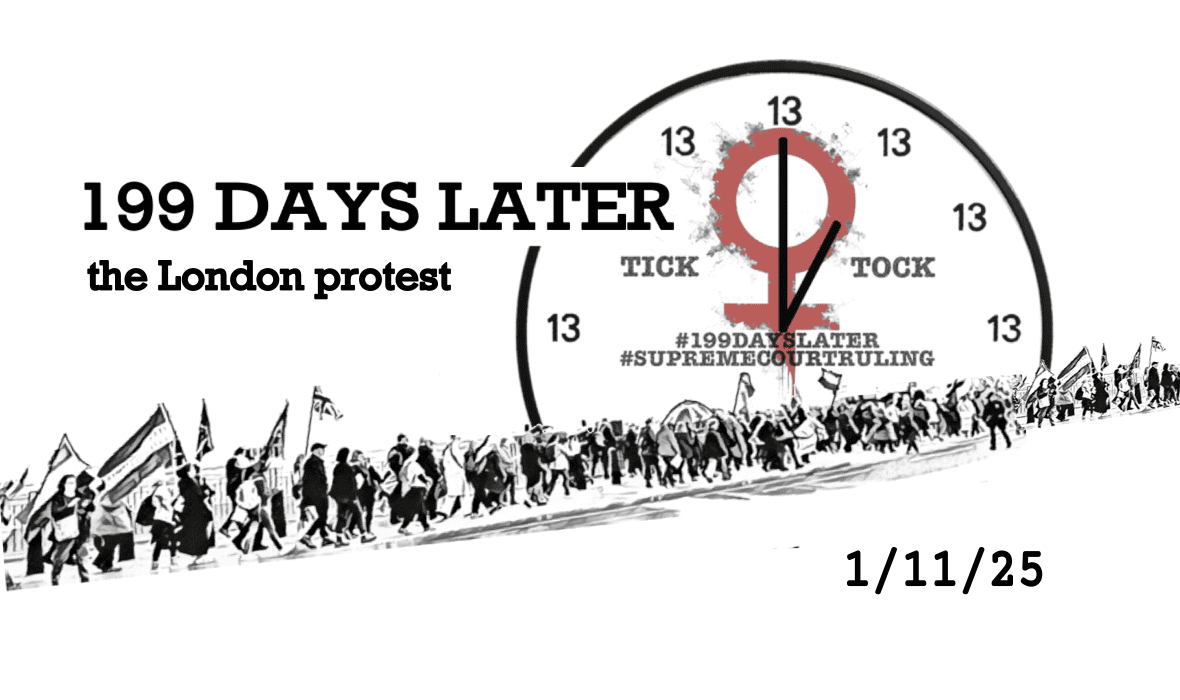
“1st November is 199 days after the Supreme Court ruling. Let’s do it then.”
It was also exactly a year on from the German Embassy protest in 2024. Although it wasn’t planned it that way, that was another great reason to do it on the first of November! When Rona from Germany agreed to send a speech to be read at the event, it all just fitted together perfectly.
The organisers were determined that the march should be for everyone, with no specific political or group allegiance required, just a shared outrage at the government’s dragging of its feet.
A Twitter account was set up in the name ‘ACTS Grassroots’. Emma came up with a subtley ’28 Days Later’ coded theme, and designed a range of leaflets, posters, flags, clock faces and tote bags. Jaydee had the idea of ordering a batch of tote bags with the logo on them. She then had the idea of asking women who were ‘known’ in the movement to pose with one. This was a great publicity plan, and the ‘199 Days Later Tote’ was popular at events like the Battle of Ideas. Voluntary contributions offered for the tote bags by a variety of people helped to pay for the fabulous flags she ordered to accompany us on the march.
Leaflets were distributed at events and protests, as well as left in libraries, coffee shops, hospitals and waiting rooms.
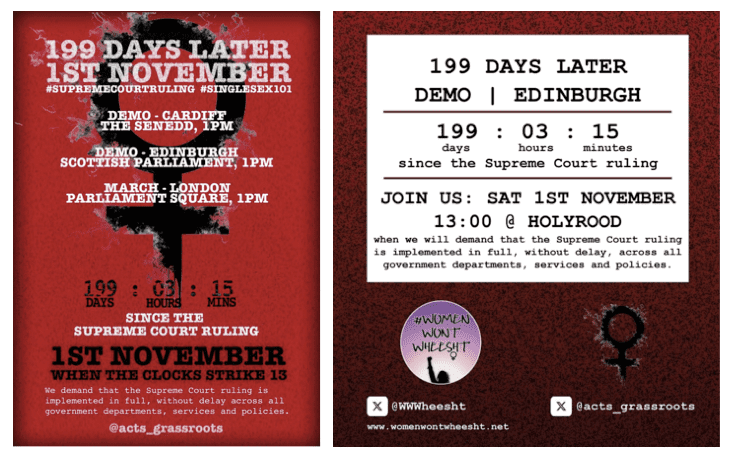
“We demand that the Supreme Court Ruling is implemented in full, without delay across all government departments, services and policies.” @acts_grassroots
. “I’m so pleased to have finally found my tribe of women who actually want to do stuff and not just talk about it. “Shall we do a march?” quickly turned into a national day of action- what a testament of how well we work together!” observed Lynsey.
“It was great being in the organising group and working with women across the country who I met via the ‘No Men in Women’s Prisons’ actions.” Ellie told me. “We were just so angry at the lack of action by our government. Personally, I just want women to matter. Despite us being the 51% we are ignored, silenced and dismissed in favour of men who say they are women. The 199 Days Later march was a chance for women to come together to say we do matter and we will not be silenced or ignored.”
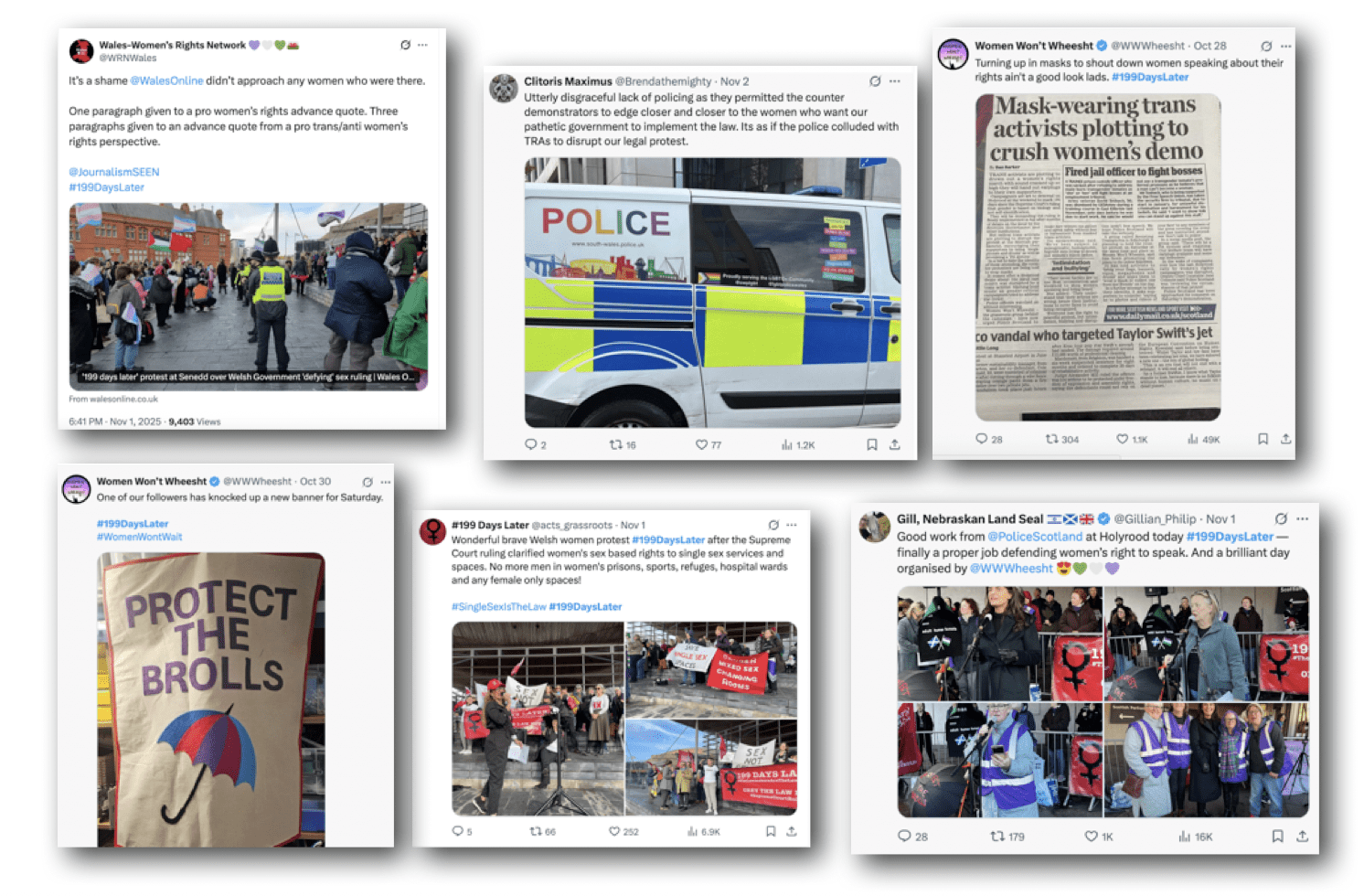
When women from Scotland and Wales contacted the organisers, saying they would organise their own protests in Cardiff and Edingburgh, they were delighted. At all three events, women and some men, from all political persuasions and walks of life, joined together to say ‘Enough’.
“Tick Tock, time is up!”
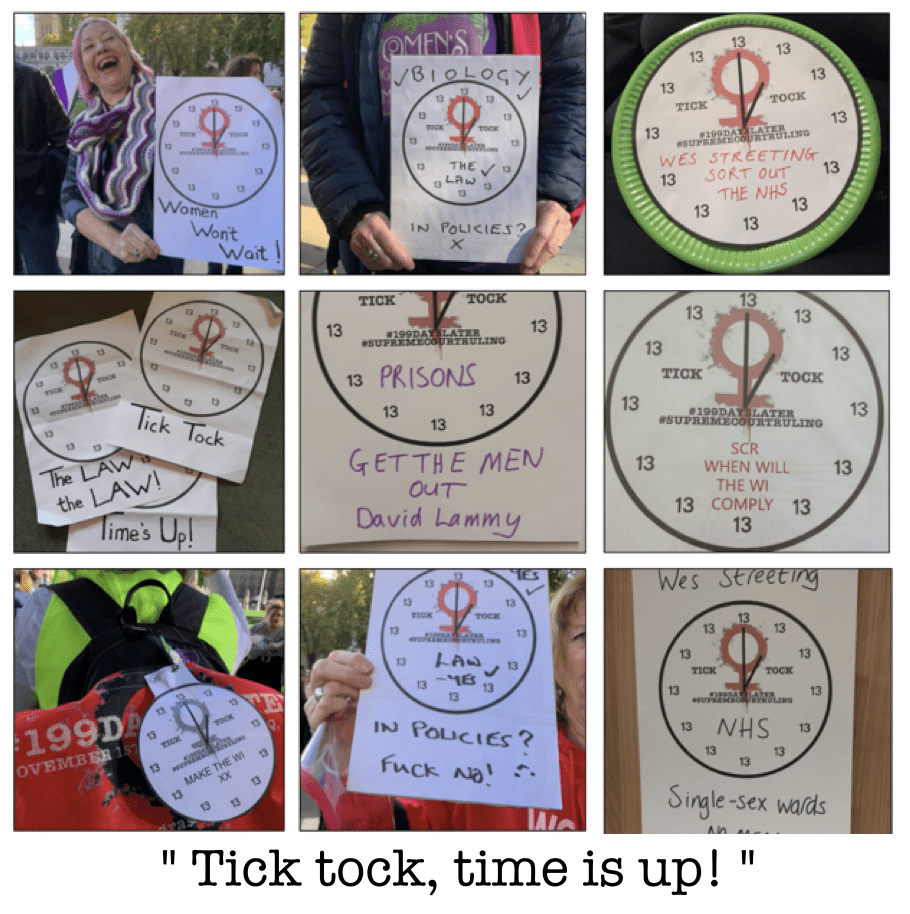
During Zoom conversations referencing 1984 and clocks striking thirteen, it was suggested women might make clock faces. Jaydee had an extensive craft stash of cardboard pizza bases that she reckoned would work perfectly and so the idea came to fruition. Emma made a promo video for Twitter, with the sound of a clock ticking loudly followed by white noise. A second video, intended to be a “rallying cry” featured vocals and a variety of women’s rights photographs.
Some women carried cardboard clocks on the march. Space was left on the templates for women to add their own messages. Women who could not attend could post their clocks on social media, and some of us posted a ‘real life’ copy to our MP.
Many women on the march held their clock faces up high as they chanted, ‘tick tock, time is up!’
A route was planned for the march, and London women checked out the planned path. Once that was decided on, Jaydee’s liaison with the police began. The police were surprisingly organised and supportive from the outset. It was decided to meet outside parliament, by the Millicent Fawcett statue and march to Downing Street, where the speeches would be held on the grass opposite. A group of women with experience stewarding was enlisted to help on the day.
People were starting to talk about the protest.
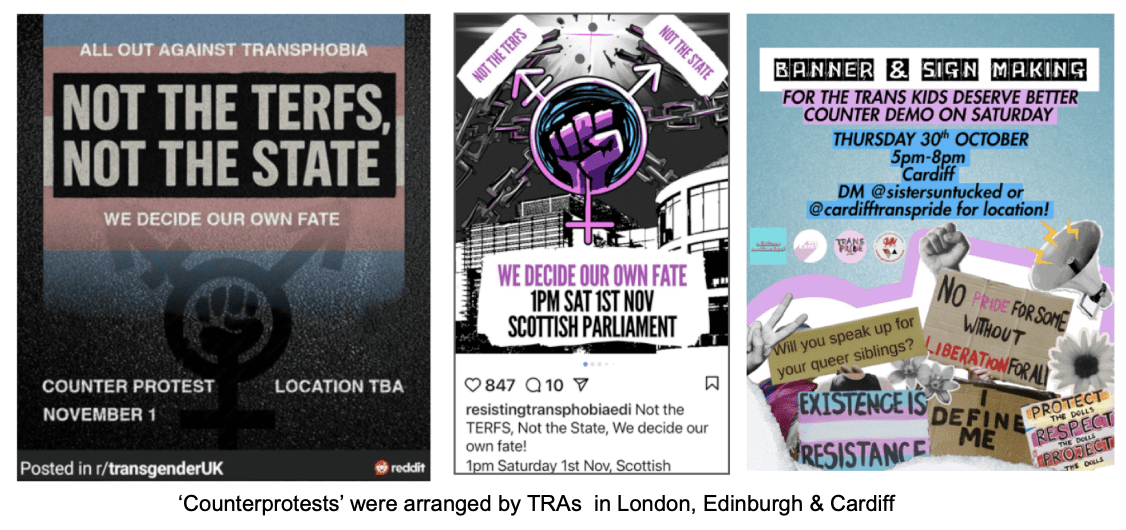
When news reached the TRAs, they were not happy. Counterprotests were organised in London, Edinburgh and Cardiff, with the catchy tagline ‘Not the TERFs, not the state, we decide our own fate’. A fate that is to be fully funded by the state, obviously, because who else is expected to pay for those pesky hormones and surgeries? Just saying.
The London protest organisers- who were mostly women North of Watford- decided to stop mentioning the march itself, focusing on the protest aspect. This turned out to be a good strategy, as it confused the TRAs, who all gathered in a park near Parliament Square and were unable to send outliers to disrupt our speeches near Downing Street.
Planning the London Speakers
“We wanted to cover a variety of areas that were affected by the government’s complacency over the Supreme Court judgement,” an organiser told me. “We were lucky to know so many amazing women that we could invite to speak. Our speakers talked about child safeguarding, schools, the NHS and private health services, women’s prisons, women’s sports, lesbian groups, the Women’s Institute, the Kenwood Ladies Pond and captured councils. We asked them to try to keep their speeches to three minutes long. They were all inspiring.”
People gather to hear the speakers opposite Downing Street
On the day
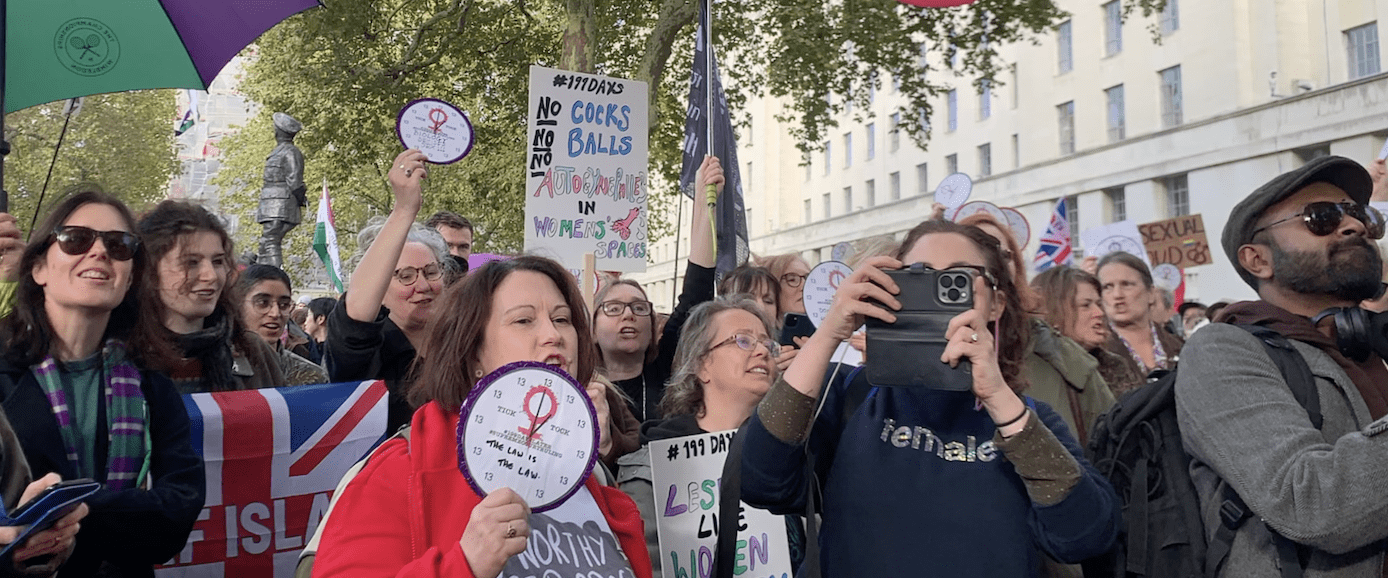
The forecast had told us to expect rain, but Saturday 1st November 2025 dawned bright and clear, which was a definite bonus. The stewards and organisers had planned to meet early at the statue, so by 11.30am a group of people had begun to gather. By twelve, with still an hour before the march was due to leave the square, the group had more than doubled. It became clear that it was going to be an excellent turn out.
As people milled around, waiting for the march to start, I asked some of the women about their reasons for attending.
“Because I don’t understand why the government, judicial system and everyone else in charge haven’t implemented what should be law. We need to raise awareness and if they don’t start making things better for women, we need to start prosecuting people for breaking the law.”
“We’re here because it’s been 199 days since the Supreme Court ruling. And still the government and other establishments aren’t bringing the ruling into practise! So the lawmakers at the moment are the lawbreakers. That’s why women are here, to tell our stories and be seen.”
“I’m here because I’m bloody angry. Yesterday we saw that the government are backing away yet again. We’re just not having it. So I’ll be raising my voice very loudly.”
“I’m here because I’m too old to go down this woowoo path. And that’s what gender is. Gender is not a thing. Sex is about biology. And I will not be led down that route- I will not!”
“The reason I’m here today is because the Supreme Court ruling makes it quite clear that in the Equality Act ‘woman’ means a biological woman- and no nonsense about men becoming women! It’s quite clear. The fact that there are so many institutions completely ignoring it is a disgrace.”
“I’m a teacher and that’s what peaked me, the language around this. Don’t ever dare call me a ‘cis’ woman! There’s no such thing. And it’s about time they put the fucking policies into place!”
“I am particularly concerned about men in women’s prisons because they are still there and we need to just be getting them all out. The women in prison are vulnerable enough as it is without men being put in there with them.”
“I work with mental health service users. Particularly quite a lot of women. A very high proportion of them have been subject to male violence- rape, domestic violence, etc- and they absolutely need single-sex spaces in order to heal from their trauma. And not to be re-traumatised.”
“It’s been 199 days and we’ve seen bugger all action. And women are not gonna wait anymore. We’ve got men in women’s prisons. We’ve got men in women’s hospital wards. We’ve got men in women’s spaces all over the place, and it’s not acceptable. Women can’t be treated like this. We say no, we do not consent!”
A woman who had never been on a protest before, told me:
“I came to my first women’s rights protest as a 62 year old because in a week where I read about the injustice meted out to the Darlington nurses, merely for requesting their legal right to single sex spaces at work, I realised just how many of our institutions are ignoring the Supreme Court ruling. It was literally a lightbulb moment for me. It’s not enough to write letters and express frustration online, I needed to be there in person, making my voice heard. I needed the powers that be to see us saying, ‘we will not back down from fighting for our legal right to single-sex spaces’.”
I spoke to Caroline who had done parkrun early that morning, before coming on to the march. She and her fellow runners had run and posed with a #199DaysLater flag and still found the energy to join the protest afterwards!
They have a Twitter thread about the march here.
“It was wonderful to be part of such a great occasion,” Caroline told me,“and combine my determination to bring fairness for women back to parkrun with my commitment to get the government to stop ignoring and sidelining the valid concerns of women who want their hard won right to single-sex spaces, sports and associations, respected. It’s the law. And it always has been.”
And then, as if by magic, it was 1pm and Big Ben began to strike. The people at the front of the march began to chant ‘tick tock, time is up!” and we were off!
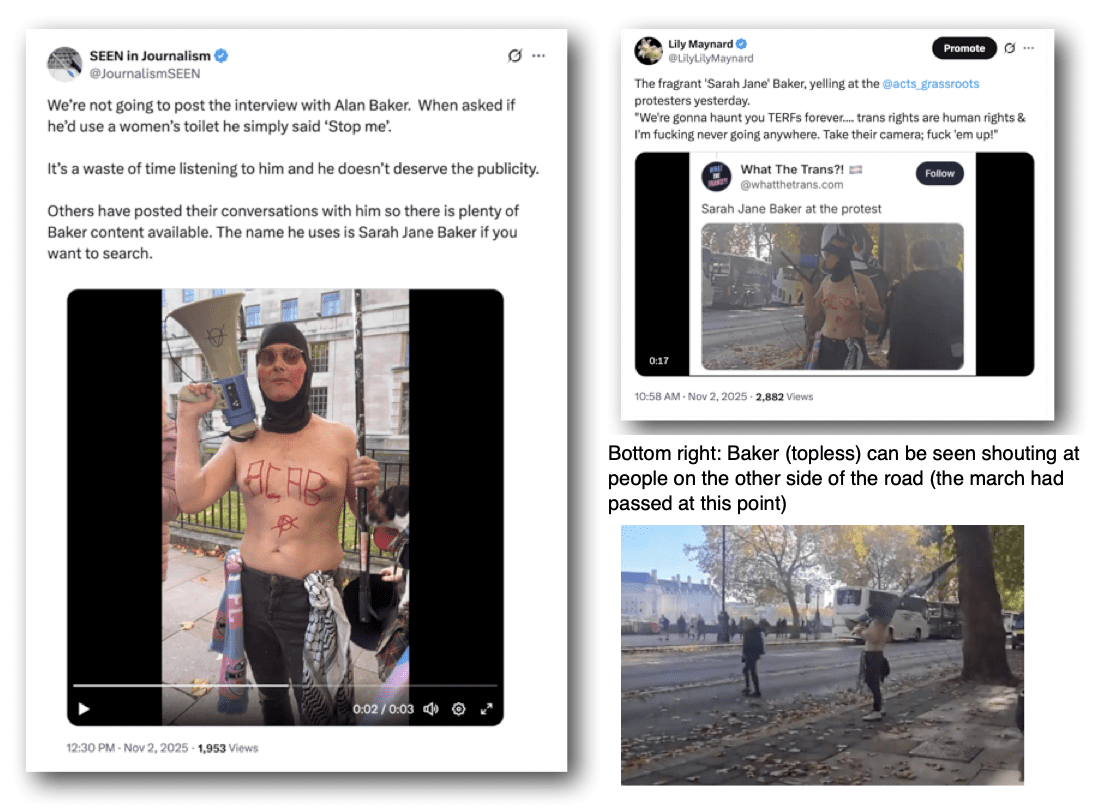
We marched from Parliament Square alongside the river and down to Downing Street. As we marched we could see the TRAs in a small park on the other side of the road. There were a couple of huge tour buses parked in front of them, so their presence was more of a minor amusement than a distraction. Unable to cause trouble with us, because the police had ‘kettled’ them inside the park, the TRAs turned on some YouTubers who were filming the whole thing, damaged a camera and a microphone (so I was told) and eventually three of them manged to get themselves arrested anyway.
Golden Boy Alan ‘Sarah Jane’ Baker was hanging out topless, happy to talk to anyone who would listen about smashing up cameras, fucking up TERFs and eating his own testicles. Luckily he was kept far away from the march, but some YouTubers did stop and chat to him. Videos can be easily found.
I’m inclined to agree with SEEN in Journalism about giving him more exposure, but I will include this quote: which is what he was shouting into a megaphone:
“We’re gonna haunt you TERFs forever…. trans rights are human rights & I’m fucking never going anywhere. Take their camera; fuck ’em up!”
“It was noticeable that a number of counter-protesters were confined on the opposite side of the street past New Scotland Yard,” one attendee told me, later. “It was a huge relief to see them pent up, well away from us, so their noisy behaviour was unable to interrupt our proceedings. The police did their job with politeness and good humour (which) made it easy for us to focus on what we wanted to achieve, a good-natured yet passionate protest.”
Protests were also taking place in Scotland and Wales
Meanwhile, the London march was approaching Downing Street. This short video posted to the @acts_grassroots account gives a rough idea of how many people attended. My guess would be 700-800.
Once we arrived at Downing Street, we established ourselves on the other side of the road to the gates. There was a wide patch of grass, overhead tree cover, and concrete around the statue.
The tall, imposing gentleman overlooking our speeches was the ‘unbeatable and unbearable’ Field Marshall ‘Monty’ Vicount Montgomery of Alermein. Not known for being the most tolerant of blokes, but you can bet he knew what a woman is. In the middle of the road, just to our right, was the far more appropriate ‘The Women of World War II’ statue.
It was the perfect place for speeches, and the TRAs were safely contained a quarter of a mile away. I stopped and looked around me. Wow. So many people and such an uplifting atomosphere. What a difference it made not to have activists waving banners, umbrellas and their little man-boobs in our faces while they screamed at us about what bigots we are.
Without a climate of fear we were able to really focus on our aims and listening to the speeches.
Andi, who organised the stewards, later told me, “the other stewards were as keen as I to offer their time, support and experience to such an important event. Jaydee had done all the police liaison so the police were aware of the potential disruption from TRAs. The energy as women and allies gathered was electric and the square was a sea of flags and banners filled with laughter and chatter. We passed the park where the protestors were gathered and being held by the police so they were unable to disrupt our progress.On reaching our destination the speeches began, and miracle of miracles, they could be heard! The police did such a good job keeping the mob at bay that every one was free to speak and be heard.”
The Speeches
After welcoming everyone to the event and joking that she wished she could refer to giant live stream screens behind us, linking us to our sister protests in Scotland and Wales, Lindsey introduced the first speaker.
“Tara was one of the organisers of last year’s action outside the German Embassy in London, standing against German self-ID law.”
Tara & Rona’s speech
“I can’t believe there are so many of you!” began Tara, looking round at the crowd.
“One year ago today, hundreds of us gathered in London outside the German Embassy… as we stood with our German sisters last year, our message to the UK was that it was not too late for us. Now, a year on, that message is more important than ever as our own government ignores the ruling of the Supreme Court.”
Tara read us out a message from Germany, from Rona of ‘was ist ein frau?’.
The Selbstbestimmungsgesetz law in Germany has meant that for the last year, anyone can change sex simply by declaration. In Berlin alone, 2,400 people have changed their legal sex, including a child under 5. Rona described this as an “erosion of women’s rights, child protection & parental authority.”
Rona gave examples of three cases which showcase what the law means in practice.
1/ A convicted far right extremist says he now identifies as a woman, and is demanding to be placed in a women’s prison.
2/ Doris Langer, who has run a women-only fitness studio for nearly 30 years, is being sued because she refused entry to a man who identifies as a woman.
3/ A family risks losing custody of their teenage son, after expressing concerns about his desire to transition. They are now fighting in court just to remain a part of their child’s life.
These are not isolated incidents. “This is the real world result of a law that claims to help a few while putting many, many more at risk.”
In the UK, she observed, we have fought hard to protect our sex-based rights but despite being defended by our Supreme Court, implementation is weak. She warned that this was how it started in Germany and that women should not compromise.
“Look at Germany and choose a different path. Women and children need protection, not ideology.”
Stephanie
“Next to speak is Stephanie Davis-Arai, founder and director of Transgender Trend; talking about child safeguarding.”
As Stephanie stepped up to the microphone, she was met with chants of “Stephanie, Stephanie! There’s only one Stephanie!”
Everybody knows what sex means, began Stephanie. The Equality Act protects women on the basis of sex, and once you let members of the male sex into the female sex category, that law becomes unworkable. ‘Stonewall lore’ has ensured that this is exactly what has happened. Since 2013, women and girls have lost many of the rights and protections given by the Equality Act. Stephanie said she wasn’t going to focus on women’s rights today, she was going to talk about girls.
“Because we often forget that the Equality Act also protects minor girls. Adolescent girls. Autistic girls. Disabled girls. Girls from all walks of life, who need these protections in society”.
It is a shame on the UK, said Stephanie, that for the last 10 years we have not safeguarded vulnerable girls. She spoke of how making public toilets both mixed adult and child, and mixed sex, leaves girls especially vulnerable. Listing a variety of situations where councils provide facilities in which girls might be vulnerable: car park or beachfront toilets, cinema or swimming pool changing rooms, the gym, the shopping centre… Stephanie drew attention to the fact that all these toilets and changing rooms are not just mixed adults and children, they are now also mixed sex.
“For the past decade we have been allowing adult men with penises to go into toilets used by young girls.”
This situation is not acceptable, concluded Stephanie. If you are a service provider, you have both an Equality Act duty to segregate your facilities by sex, and a safeguarding duty to protect girls.
Jennifer
“Next to speak is Jennifer Gourley from Protect and Teach, who will speak about why schools have abandoned safeguarding in order to protect men who think putting on a dress makes them a woman.”
Protect and Teach, Jennifer told us, is concerned with how schools are being ill-advised about the legality of allowing male teachers, and schoolboys, to claim they are female. Prior to April 2025 schools at least had the excuse of being ill-advised, but that lack of clarity no longer exists and hasn’t existed for 199 days.
“Why then, when a male teacher appears in a school in a dress, are schools still insistent that children refer to him as ‘Miss’?”
Far from doing no harm, this tells children, both boys and girls, that being a woman is just a feeling rather than a biological reality. It erases girls’ boundaries, safety, and privacy from the male gaze. Children should “not be expected to validate a teacher’s sexually-stimulated immersive role play”. This is a form of emotional abuse. Schools have a statutory duty to provide a safe environment; instead they are deliberately creating a special caste of teachers that cannot be questioned. Such a policy not only teaches children that “authority trumps truth”, it sidelines their welfare. Schools are meant to abide by the statutory guidance, but they are not doing so.
“They’ve had 199 days to bring back common sense and safeguarding. Why are they dragging their feet?”
Dr Alice
“Next up is Doctor Alice, a GP in Cambridge working in urgent care, and a founding member of the group Biology in Medicine, which campaigns to reduce harm to trans-identified people.”
Alice said she often saw trans-identifed people in urgent care, “and it breaks my heart to see the harms to these people that have been done by my profession. It’s absolutely shameful that the NHS is doing this to people. And it’s not just the NHS, it’s private providers as well.”
Dr Alice described herself as “angry at my profession and dismayed that this is happening”. What people who are trans-identifying don’t seem to understand, she continued, is that they won’t be accepted in their adopted gender. You are the sex you were born, in reality and for the purpose of the Equality Act, and we should not be lying to people.
“The Supreme Court judgement should have stopped this happening. There are so many abusive things that are happening to people. Biology in Medicine is calling out the NHS and all medical establishments.
“Because transition is a lie. We are lying to people!”
Judith
The next speaker, Lynsey announced, was Judith, “a women’s rights campaigner, who will tell us about the situation with prisons.”
“The government is still defying the law by keeping women locked up with men,” began Judith. She went on to state that there are twelve prisons accommodating convicted women in England and Wales, yet we don’t know how many men are held in these prisons or which prisons they are all held in.
“We do know that these men include… Lauren Jeska!”
And at this point, Venice whipped out a larger than life-size portrait of the Park Run stabber and handed it to Ellie who held it aloft.
“Lauren Jeska!” called out Judith.“Real name Michael Jameson. Convicted of attempted murder.”
left to right: John ‘Sally’ Dixon, Kyle ‘Zoe’ Watts, Michael ‘Lauren Jeska’ Jameson
“Not our crimes, not our crimes!” from women in the crowd.
“We believe that he is in Askham Grange now,” continued Judith.
Venice held another larger-than-life photo up high.
“Sally Dixon! ” called Judith. “Real name John Dixon. Convicted of sexually abusing children. He is in Bronzefield prison.”
A third picture appeared.
“ Zoe Watts! Real name, Kyle Watts.”
“Boo, boo!” from the crowd.
“Watts is a former police community support officer, no less. He is in Downview Prison, jailed for arms offences!”
“He’s a man, he’s a man!” came a cry.
Judith explained that members of the Labour government, including the current prisons minister, James Timpson, have repeatedly claimed, falsely, that E wing at Downview is not part of the general women’s estate. We must not be fooled into thinking that this is acceptable. Any prison which houses even one man is a mixed prison, and all male prisoners need to be moved into the male estate as a matter of urgency. David Lammy’s reply, when asked if he accepted the Supreme Court ruling, that he “strongly believed that trans people’s safety and well-being must be protected”, was a ‘slap in the face’ to women, said Judith. Vulnerable women prisoners “could easily be forgotten, subject to the whim of government ministers” and she asked that people write to their MP to protest.
The dangers of placing male prisoners with women was acknowledged in British law in 1823. That people are hell bent on dragging the rights of women prisoners back 200 years is quite frankly terrifying.”
“Follow us on X and on YouTube at @NoMinWPrisons. And follow the hashtag #NoMenInWomensPrisons.”
Before introducing the next speaker, Lynsey told us that the previous week she had had the pleasure of meeting the Darlington nurses, and Sandie Peggie. Everybody cheered. She called them “brave, brave women hung out to dry by their unions”.
Teresa
Next up we have Teresa Steele,” announced Lynsey. “Teresa is a longstanding campaigner for same-sex wards and same-sex care in the NHS.”
“It is such an honour to be invited to speak here today. Thank you. I’m here to talk about the collapse of sex-based boundaries in the NHS. Successive governments have turned a blind eye while NHS subversives have systematically dismantled essential single sex spaces and care.”
Teresa believes the NHS is no longer a safe environment for women and girls, as policy corruption “has spread like contagion across NHS trusts nationwide.” In support of this view she points out that between 2019 and 2022, there were over 6500 sexual assaults and rapes on NHS premises.
Calls of “Shame, shame!” from the audience.
Despite the Supreme Court ruling, this government refuses to do its job and ensure that the NHS operates within the law.
“Women are fully entitled to expect that women-only wards contain only women!”
Teresa pointed out that the policy “which allows predatory men onto our wards” is unlawful. Women should not be coerced into accepting same-sex intimate care from female impersonators, nor should they be forced to share their single sex changing rooms with men.
“To NHS Fife and Darlington- a plague on both your houses! And to Bridget Phillipson, I say – none of these dangerous and discriminatory measures could have passed a properly conducted Equality Impact Assessment in the first place!”
Women will continue to fight back, as more and more people start to realise that these unlawful policies could harm any one of their female friends or relatives.
“And like the Supreme Court judgement, we shall prevail!”
Rose
“Our next speaker is Rose Reeves, who is going to talk about the impact of the Supreme Court judgement on one particular lesbian group. Please welcome- Rose.”
When he announced the Supreme Court judgement, Lord Hodge referred to a submission made by the Lesbian Interveners. They were Scottish lesbians, the Lesbian Project and LGB Alliance, and we send them our thanks! Lord Hodge said that their evidence portrayed, and I quote, “a chilling effect on lesbians who are no longer using lesbian-only spaces because of the presence of transwomen.”
A group called Older and Wilder, a social group for older lesbians in Bradford, is experiencing that chilling effect right now, and had asked Rose to speak on their behalf.
Older and Wilder has been meeting since 2007. They met at a local LGBT organisation called the Equity Partnership. However. At some point, the equity partnership changed its constitution to become ‘trans inclusive’ and told Older and Wilder that all the groups that met there also had to become trans inclusive. The groiup complied, but lost members over the years. Some women felt uncomfortable, but stayed because they valued being in the group. In the light of the Supreme Court ruling the group realised they were perfectly entitled to be a ‘female born’ lesbian group, and challenged the Equity Partnership, which responded by claiming Older & Wilder never was a single sex group, that the legal situation was complicated and transwomen are women. Finally, it said “if you don’t like it, you’re free to go elsewhere.”
The Equity Partnership made two big mistakes, said Rose. Firstly, putting ‘all this legal gobbledygook down in writing’ and secondly, underestimating “the power of lesbians when they are roused to action!”
Rose told us that the story did not yet have an ending, but the aptly-named Older and Wilder group is fighting back against this ‘lesbophobic lawbreaking’ with the Supreme Court on their side.
Alison
“Next up we have Alison Jenner, here to talk about the situation with the Women’s Institute.”
Rose talked about the impact on one small association, began Allison. I’m going to focus on one big association: the Women’s Institute, which was founded in 1915 in the UK. The point of the WI was for women to learn new skills from women just like themselves, and to help each other and work together for the for the public good. In 1953, the WI was the largest women’s movement, with members totaling over. 446,000. Now membership is around 205,000. Seeking for growth and trying to appeal to younger, more diverse groups, the WI could have used its women-only membership as a draw to groups where single sex meetings were a plus; “women in diverse neighbourhoods could have shared their skills with ours and their traditions with ours”. But instead the national leadership decided to include ‘special men’. They claim ‘transwomen’ have been joining since the 70s, although Alison had been able to find no proof of this.
There is no record of male members- they could be in the low dozens to the few hundreds, although the WI Constitution explicitly limits membership to ‘women who have reached the age of majority’. In 2021 Alison received the new EDI policy, which she described as, “nine pages of of badly digested and regurgitated misunderstanding of the Equality Act.”
While the policy states, “the Women’s Institute lawfully restricts membership to women only”, it also includes over a page about how transgender and non-binary members are welcome to join, “in the same way as any other woman”.
In addition, to ask for a GRC is not considered acceptable.
“This EDI Plus policy is incompatible with the WI’s Constitution and with the Supreme Court ruling. Admitting males dilutes the charitable purposes of the WI by shifting resources and focus away from biological women’s unique needs”.
It especially affects discussions on issues such as reproductive health, menopause and sex-based violence. Women from certain ethnic groups who might have wanted to join may not now, because the organisation is not single sex. In addition, women who are sex realists may feel they can’t join. The policy is damaging the organisation’s reputation and the WI should suspend the admission of trans-identified men and revise its EDI policy to define women as biological females.
“The WI must comply!”
Venice
“Next up, we have Venice Allan, agitator, organiser and activist, talking about the Hampstead Women’s Pond.”
Venice said hello and told us she would try to not fall off the step ladder. She reminded us it was199 days since the Supreme Court ruled what a woman is and 100 years since women got their own ‘women only’ swimming pond on Hampstead Heath. There are three ponds on the Heath, but these men don’t want to use the mixed pond. They want to take over women’s spaces.
“Wherever there is a sign where it says ‘women only’, we know there will be men crying and lying to be let in. And there is no more iconic or historic women’s space than the Kenwood Ladies Pond, and that’s why they want it so much!… Every single thing that women have built for ourselves, they want to destroy.”
The City of London sham consultation is a joke, said Venice, and women are not going to let them get away with it. Sex Matters is taking them to court and Sex Matters will win. Where it says women only, men are not welcome.
“And as our sisters in Scotland are saying right now, ‘women won’t wheesht’. I don’t know how to say wheesht in Welsh, but I know women across Britain are coming out today because we won’t shut up. We will keep on speaking and meeting and marching, again and again, until every single women’s space and service in this beautiful country is rid of men!”
Everyone clapped & cheered a lot.
Cath
“Next up we have Cath Dyson, women’s rights campaigner. Here to talk about the captured councils.”
“Go on, Cath!” shouted someone.
Cath thanked the organisers and said Venice would be a hard act to follow.
Local authorities are responsible for the delivery of vital services to residents, she reminded us, including “children’s services, education, leisure services, provision of rape and domestic violence services and accommodation for vulnerable or homeless women.” Yet several councils have a formal statement that says ‘trans women are women’ and have introduced self ID into their services. These councils include Cambridge, Manchester, Norwich, Hackney and Bristol, where recently 10 Green councillors walked out of a council meeting after residents asked about the rights of women.
Cath told us she was involved in work to find out which local authorities are responding to the Supreme Court judgement.
“What I’ve seen doesn’t fill me with any confidence.”
Of a hundred and seventeen English councils, half are ‘waiting for guidance’. So there is no policy review, an no training review, even though the law is the law and any guidance does not change that. A quarter of these councils have sent out staff communications; only a handful saying anything about sex-based rights and women. Most focus on ‘inclusivity’ with no mention of women, lesbian or female. Councils seemed more concerned with how stressful and complicated the ruling is for trans-identified people. Essex County Council said, “there is no urgent action for us to take in response to this decision (it) doesn’t make anything we do obviously illegal although it may increase litigation.”.
The Council goes on to make it clear that it is happy for there to be an increased risk and the risk is to women. Stroud Council says they “want to make it clear to trans, intersex and non-binary staff and residents whose lives have been thrown into uncertainty that this council is committed to ensuring everyone feels safe”. But not women, of course. “There is no recognition that the rights of women may have been compromised. It is almost like we don’t matter.”
Cath says she has worked in these organisations and knows the time and effort it takes to draft these communications. Councils will have to be “dragged kicking and screaming to follow the law and provide female only services”. We must not let up the pressure on our councils. This is a call to action for you. Write to your councillors, find out who the Chief Executive is.
“Make sure that they know that you know the law and demand that they follow it!”
Tish
“Our penultimate speaker is Tish. She has been in this fight for 10 years, to save her son from medicalisation and to defend single sex spaces for women and girls.”
Tish told us that her son came out as trans after coming out as gay. His parents suspected he might turn out gay as a little boy, “although he could have turned out to be a heterosexual man who liked theatre!” Despite his parents’ acceptance, at school he was bullied badly from a young age and called names like ‘faggot’. In consultation with the school, it was arranged that he should not have to use the male toilets, and that he could skip playing sports with the boys, “because that’s where his homophobic bullying took place.” Tish would not have been happy for her son to invade girls’ spaces, but provision was made without that, and her son never asked. This, she said, shows that vulnerable boys can be treated with sensitivity, without imposing on girls spaces.
“Now I’m his mum, I think he’s lovely. I would say that because I’m his mum. But if you let my son in (to women’s spaces), you’ve got to let every other man in.”
Tish also wanted to speak about the fact that she is a woman with five sisters, and that sexual offence statistics are ‘written on the bodies of my sisters’. Sexual assault on the way to school as a child left Tish’s older sister struggling with morbid obesity all her life and absolutely terrified of men.
“For my sister, single-sex spaces mattered. But I should also say you should not have to have a history of sexual abuse to have the right to single-sex spaces.”
She concluded by saying she hoped the medical profession was shamed by what they were doing to the healthy bodies of gay boys like her son, prescribing harmful drugs that caused helth issues and adding to their confusion. “You’re painting a target on his back. He’s gay, he’s confused, he’s been groomed, he’s been manipulated.”
Tracy
“Our final speaker today is Tracy Edwards, round the world sailor and women’s rights activist. Please welcome Tracy!”
“I’m used to climbing masts and all sorts!” joked Tracy as she mounted the step ladder. “I’ve been told to make this short and sweet because apparently you all want to go to the pub.”
Tracy said she always thought that sport would be the thing that would ‘crack the nut’ and ‘sort this mess out’.
“We see big male bodies next to small female bodies in sport and it is so obvious. It is so visual, it’s so visceral.”
After watching the world cheer as two men ‘beat the living daylights out of two women’ in the Olympics in 2024, Tracy knew we were in real trouble.
“Anyone who pointed out that they were men was threatened and abused. I just couldn’t believe it.”
Some sports, like Rugby, did the right thing before the Supreme Court ruling. And others have done the right thing since. But even though sports governing bodies may adhere to the law, there are still clubs that completely ignore the governing bodies adherence. For example, British Rowing complied with the law ages ago. But it is only just in the last few days have Cambridge University complied.
“Sport is played with the physical bodies of men and women. It is not played with feelings. And as much as I would love to be inclusive and take everyone on board Maiden (her boat), it’s just not possible- it’s a very small boat! We can’t be inclusive in sport because sport is about safety. And fairness.”
There are thirty four sports in England alone that are flouting the law. It is depressing how easy it was to strip away the rights that women fought for. Sports governing bodies’ actions are dismissive of women’s right to fair and safe sport.
“No one is saying that trans people cannot play sport. We are simply saying everyone must compete in the category to which their body belongs.”
Tracy told us that she and Sharron Davies are currently working on an initiative which will involve tackling these governing bodies, and they will be providing resources online to help other women get involved. Tracy told us that Sharron gets hundreds of emails and letters from mothers who don’t want boys in their daughters’ school sports teams. They’ve had enough. “We’re going to start holding some feet to some fires!” Tracy and Sharron are going to be talking to Insurance companies, she said, who may not know that they’re about to be liable for a lot of lawsuits. What will it take for them to wake up, she asked. A broken neck? A death?
“Kier Starmer, do your job! We’ve had enough. This is the hill that I will die on. The law is the law! Women want our stuff back!”
She concluded to cheers. Another chant of ‘tick tock, time is up!” was struck up, after which we sang the For Women Scotland ‘Women’s Rights’ song, before dispersing to the pub.
“For women’s rights are human rights
We won’t let you forget
For women’s rights are human rights
This isn’t over yet.”
Videos of the speeches
You can watch videos of all the individual speeches in full on this thread on the @acts_grassroots account on Twitter.
Finally, a thought from another of the organisers. “The legal rulings can often mean that women step back from doing the activism we’ve started. They step back because they think these rulings mean we’ve won. It can start to feel like we’re being thrown bread crumbs on a bird table, to shut us up and appease us. You think things are going to change, but nothing really changes until women start coming out en masse. No doubt we’re going to have to do it again and again, and again, but we will not be stopping!”
Post Script
Miles to go before we sleep
As I finish up this article, nearly two weeks after the London protest, one of the organisers sends a message on WhatsApp. “We’re in the Times!” Sure enough, the Times mentions 199 Days Later in an article dated Friday 14th November.
“Civil servants were told women’s rights demonstrations were “anti-trans”, according to a leaked email.
The email, seen by The Times, showed the Cabinet Office warned staff about an “anti-transgender rights” protest taking place on November 1.
“It is thought to refer to the 199 Days Later march in London, Cardiff and Edinburgh, to highlight that public bodies had yet to align their policies, including on single-sex spaces, with equality law… Whitehall sources suggested the warning risked breaching impartiality rules and reflected a reluctance among civil servants to implement the judgment.”
It seems we may have some way to go yet.
But we won’t be going quietly. And we will not be stopping.

 Why did we need a protest?
Why did we need a protest?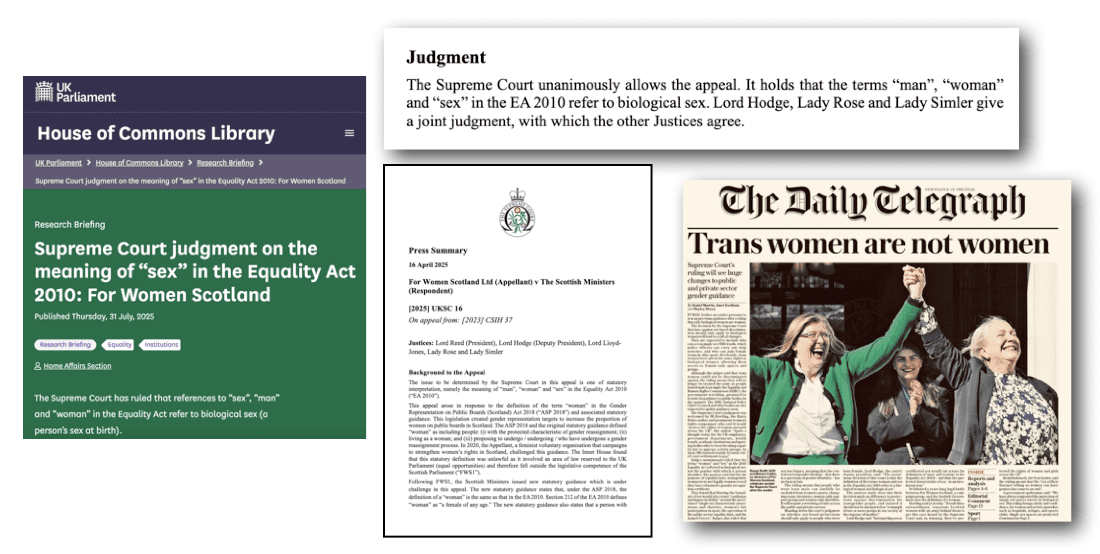
 That we needed the highest court in the land to tell us what a woman is, is in itself both surreal and absurd. That even after the aforementioned court had spoken, people would claim the ruling was ‘difficult’ or ‘complicated’ shows just what a grip gender ideology has on the collective bollocks of our culture. That the government would drag its feet after such a ruling should be, quite frankly, unbelievable.
That we needed the highest court in the land to tell us what a woman is, is in itself both surreal and absurd. That even after the aforementioned court had spoken, people would claim the ruling was ‘difficult’ or ‘complicated’ shows just what a grip gender ideology has on the collective bollocks of our culture. That the government would drag its feet after such a ruling should be, quite frankly, unbelievable. 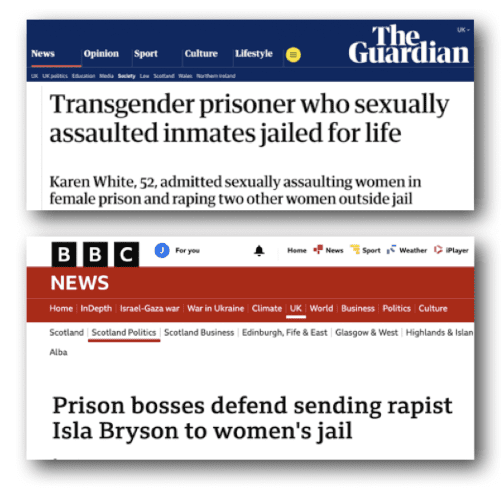
 In 2024 Philipson said someone who had gone through ‘quite an extensive process’ to ‘change gender’ should be allowed to use the toilets of their ‘aquired gender’. After the Supreme Court ruling in April, she changed her tune. Nothing has actually been done, however.
In 2024 Philipson said someone who had gone through ‘quite an extensive process’ to ‘change gender’ should be allowed to use the toilets of their ‘aquired gender’. After the Supreme Court ruling in April, she changed her tune. Nothing has actually been done, however.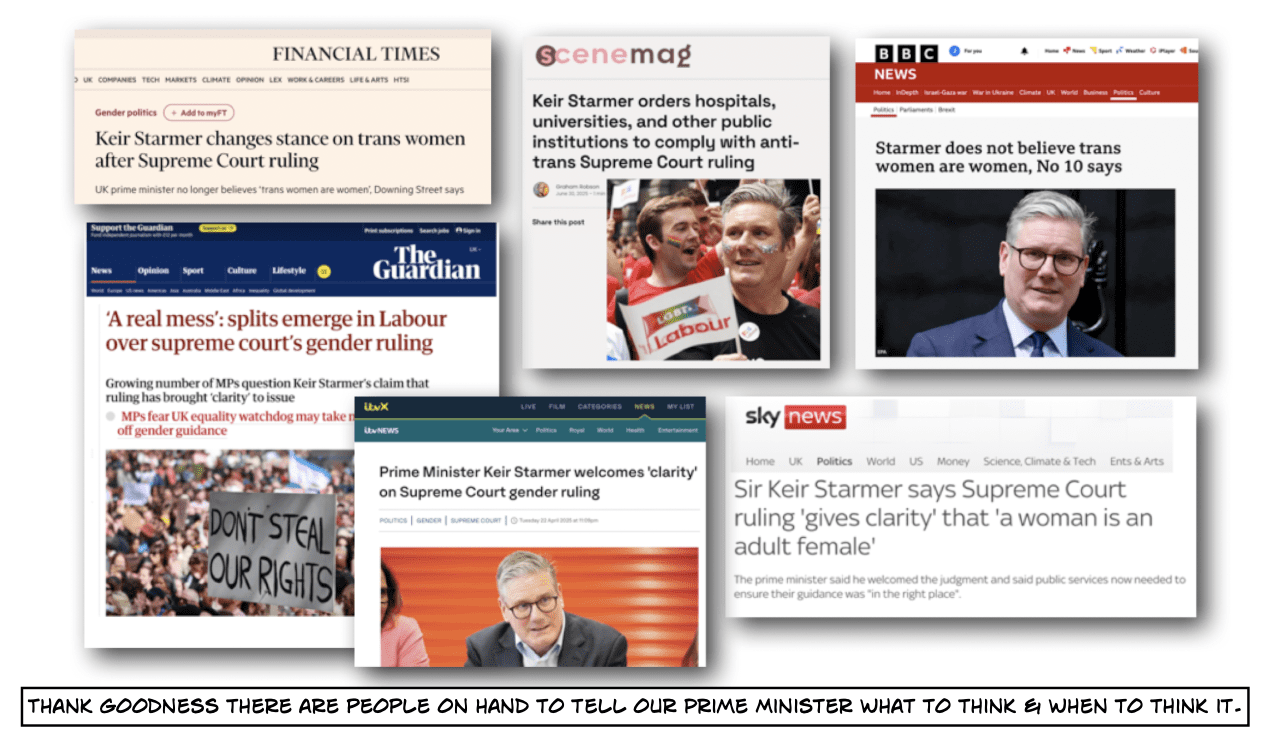
 It was in this post-Supreme-Court-ruling climate, that a small group of women from all over England began discussing how they might organise something the government would have to notice; something to shame our politicians and let them know we are watching. The government needed to be held to account- at very least it needed a bloody good telling off. A
It was in this post-Supreme-Court-ruling climate, that a small group of women from all over England began discussing how they might organise something the government would have to notice; something to shame our politicians and let them know we are watching. The government needed to be held to account- at very least it needed a bloody good telling off. A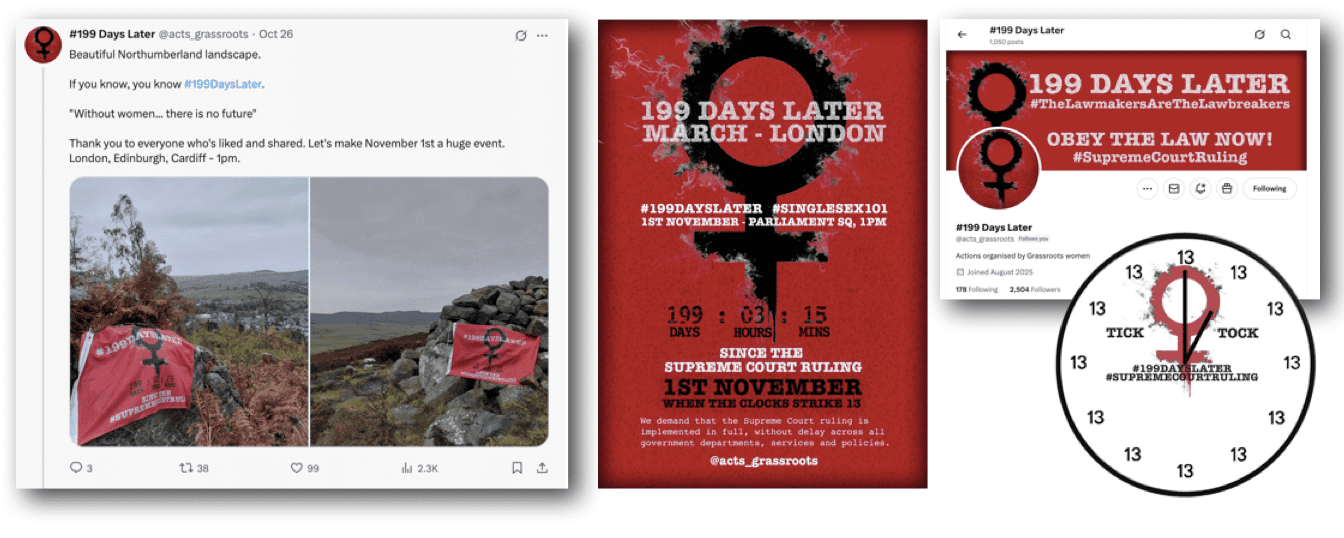

 “It
“It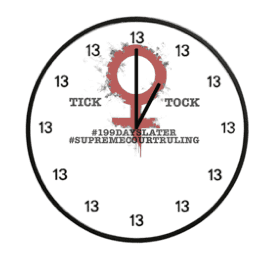 During Zoom conversations referencing 1984 and clocks striking thirteen, it was suggested women might make clock faces.
During Zoom conversations referencing 1984 and clocks striking thirteen, it was suggested women might make clock faces. 

 “We’re here because it’s been 199 days since the Supreme Court ruling. And still the government and other establishments aren’t bringing the ruling into practise! So the lawmakers at the moment are the lawbreakers. That’s why women are here, to tell our stories and be seen.”
“We’re here because it’s been 199 days since the Supreme Court ruling. And still the government and other establishments aren’t bringing the ruling into practise! So the lawmakers at the moment are the lawbreakers. That’s why women are here, to tell our stories and be seen.”
 “I am particularly concerned about men in women’s prisons because they are still there and we need to just be getting them all out. The women in prison are vulnerable enough as it is without men being put in there with them.”
“I am particularly concerned about men in women’s prisons because they are still there and we need to just be getting them all out. The women in prison are vulnerable enough as it is without men being put in there with them.” I spoke to Caroline who had done parkrun early that morning, before coming on to the march. She and her fellow runners had run and posed with a #199DaysLater flag and still found the energy to join the protest afterwards!
I spoke to Caroline who had done parkrun early that morning, before coming on to the march. She and her fellow runners had run and posed with a #199DaysLater flag and still found the energy to join the protest afterwards! 

 The tall, imposing gentleman overlooking our speeches was the ‘unbeatable and unbearable’ Field Marshall ‘Monty’ Vicount Montgomery of Alermein. Not known for being the most tolerant of blokes, but you can bet he knew what a woman is. In the middle of the road, just to our right, was the far more appropriate ‘The Women of World War II’ statue.
The tall, imposing gentleman overlooking our speeches was the ‘unbeatable and unbearable’ Field Marshall ‘Monty’ Vicount Montgomery of Alermein. Not known for being the most tolerant of blokes, but you can bet he knew what a woman is. In the middle of the road, just to our right, was the far more appropriate ‘The Women of World War II’ statue.
 After welcoming everyone to the event and joking that she wished she could refer to giant live stream screens behind us, linking us to our sister protests in Scotland and Wales, Lindsey introduced the first speaker.
After welcoming everyone to the event and joking that she wished she could refer to giant live stream screens behind us, linking us to our sister protests in Scotland and Wales, Lindsey introduced the first speaker.


 It is a shame on the UK, said Stephanie, that for the last 10 years we have not safeguarded vulnerable girls. She spoke of how making public toilets both mixed adult and child, and mixed sex, leaves girls especially vulnerable. Listing a variety of situations where councils provide facilities in which girls might be vulnerable: car park or beachfront toilets, cinema or swimming pool changing rooms, the gym, the shopping centre… Stephanie drew attention to the fact that all these toilets and changing rooms are not just mixed adults and children, they are now also mixed sex.
It is a shame on the UK, said Stephanie, that for the last 10 years we have not safeguarded vulnerable girls. She spoke of how making public toilets both mixed adult and child, and mixed sex, leaves girls especially vulnerable. Listing a variety of situations where councils provide facilities in which girls might be vulnerable: car park or beachfront toilets, cinema or swimming pool changing rooms, the gym, the shopping centre… Stephanie drew attention to the fact that all these toilets and changing rooms are not just mixed adults and children, they are now also mixed sex.

 Alice said she often saw trans-identifed people in urgent care, “a
Alice said she often saw trans-identifed people in urgent care, “a


 The dangers of placing male prisoners with women was acknowledged in British law in 1823. That people are hell bent on dragging the rights of women prisoners back 200 years is quite frankly terrifying.”
The dangers of placing male prisoners with women was acknowledged in British law in 1823. That people are hell bent on dragging the rights of women prisoners back 200 years is quite frankly terrifying.”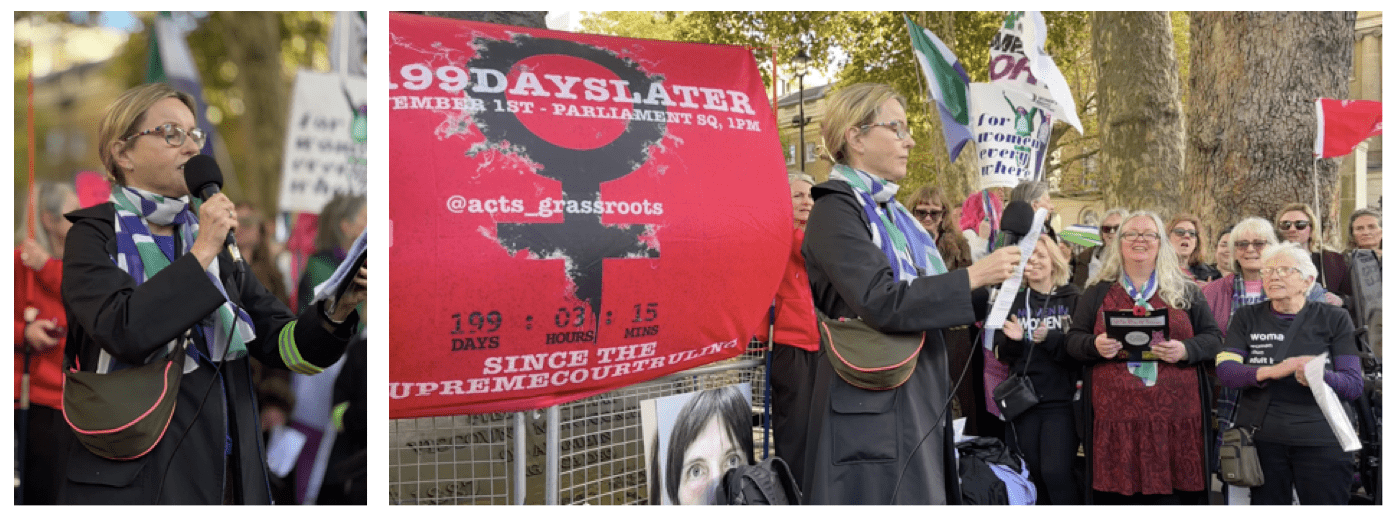
 Teresa pointed out that the policy “which allows predatory men onto our wards” is unlawful. Women should not be coerced into accepting same-sex intimate care from female impersonators, nor should they be forced to share their single sex changing rooms with men.
Teresa pointed out that the policy “which allows predatory men onto our wards” is unlawful. Women should not be coerced into accepting same-sex intimate care from female impersonators, nor should they be forced to share their single sex changing rooms with men.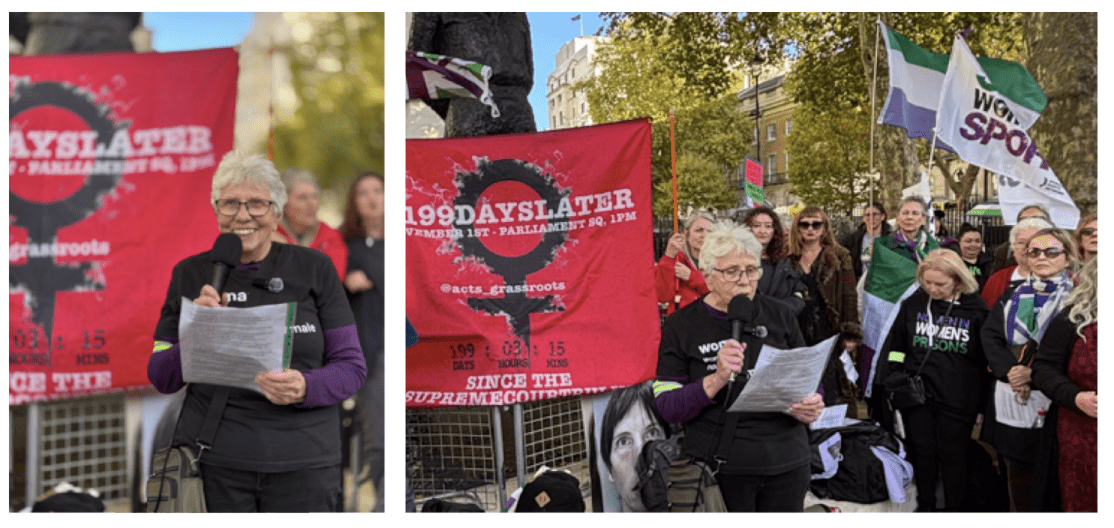 When he announced the Supreme Court judgement, Lord Hodge referred to a submission made by the Lesbian Interveners. They were Scottish lesbians, the Lesbian Project and LGB Alliance, and we send them our thanks! Lord Hodge said that their evidence portrayed, and I quote,
When he announced the Supreme Court judgement, Lord Hodge referred to a submission made by the Lesbian Interveners. They were Scottish lesbians, the Lesbian Project and LGB Alliance, and we send them our thanks! Lord Hodge said that their evidence portrayed, and I quote,  Partnership, which responded by claiming Older & Wilder never was a single sex group, that the legal situation was complicated and transwomen are women. Finally, it said “if you don’t like it, you’re free to go elsewhere.”
Partnership, which responded by claiming Older & Wilder never was a single sex group, that the legal situation was complicated and transwomen are women. Finally, it said “if you don’t like it, you’re free to go elsewhere.”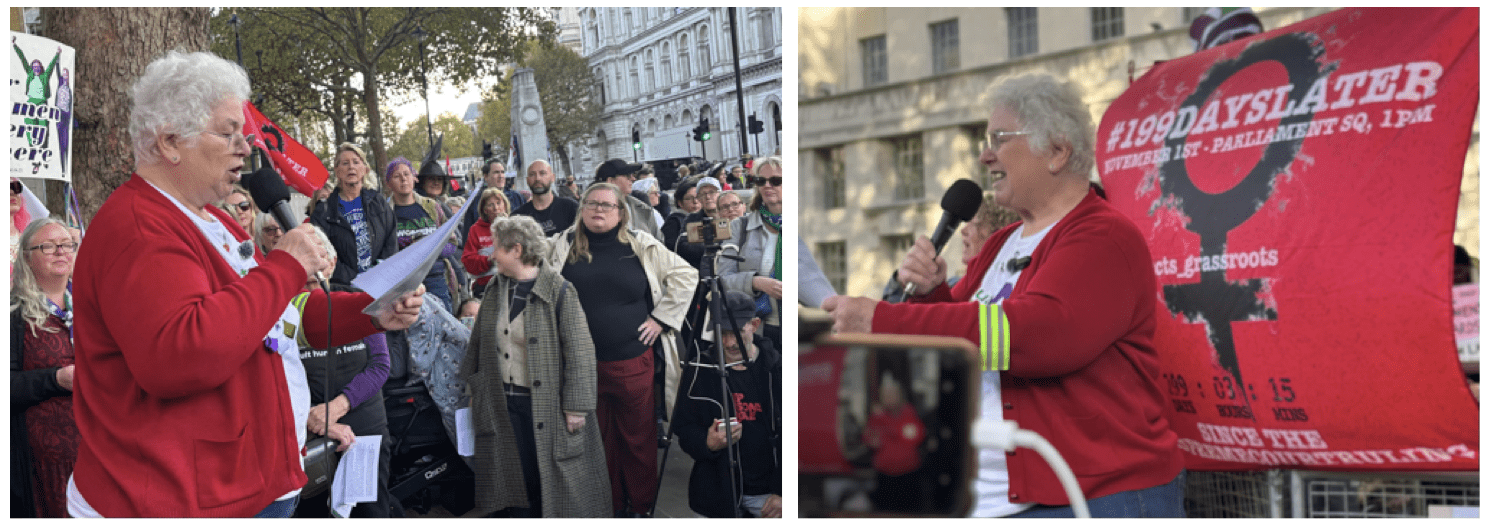 Rose talked about the impact on one small association, began Allison. I’m going to focus on one big association: the Women’s Institute, which was founded in 1915 in the UK. The point of the WI was for women to learn new skills from women just like themselves, and to help each other and work together for the for the public good. In 1953, the WI was the largest women’s movement, with members totaling over. 446,000. Now membership is around 205,000. Seeking for growth and trying to appeal to younger, more diverse groups, the WI could have used its women-only membership as a draw to groups where single sex meetings were a plus; “women in diverse neighbourhoods could have shared their skills with ours and their traditions with ours”. But instead the national leadership decided to include ‘special men’. They claim ‘transwomen’ have been joining since the 70s, although Alison had been able to find no proof of this.
Rose talked about the impact on one small association, began Allison. I’m going to focus on one big association: the Women’s Institute, which was founded in 1915 in the UK. The point of the WI was for women to learn new skills from women just like themselves, and to help each other and work together for the for the public good. In 1953, the WI was the largest women’s movement, with members totaling over. 446,000. Now membership is around 205,000. Seeking for growth and trying to appeal to younger, more diverse groups, the WI could have used its women-only membership as a draw to groups where single sex meetings were a plus; “women in diverse neighbourhoods could have shared their skills with ours and their traditions with ours”. But instead the national leadership decided to include ‘special men’. They claim ‘transwomen’ have been joining since the 70s, although Alison had been able to find no proof of this.
 Venice said hello and told us she would try to not fall off the step ladder. She reminded us it was199 days since the Supreme Court ruled what a woman is and 100 years since women got their own ‘women only’ swimming pond on Hampstead Heath. There are three ponds on the Heath, but these men don’t want to use the mixed pond. They want to take over women’s spaces.
Venice said hello and told us she would try to not fall off the step ladder. She reminded us it was199 days since the Supreme Court ruled what a woman is and 100 years since women got their own ‘women only’ swimming pond on Hampstead Heath. There are three ponds on the Heath, but these men don’t want to use the mixed pond. They want to take over women’s spaces.
 “Go on, Cath!” shouted someone.
“Go on, Cath!” shouted someone. The Council goes on to make it clear that it is happy for there to be an increased risk and the risk is to women. Stroud Council says they “want to make it clear to trans, intersex and non-binary staff and residents whose lives have been thrown into uncertainty that this council is committed to ensuring everyone feels safe”. But not women, of course.
The Council goes on to make it clear that it is happy for there to be an increased risk and the risk is to women. Stroud Council says they “want to make it clear to trans, intersex and non-binary staff and residents whose lives have been thrown into uncertainty that this council is committed to ensuring everyone feels safe”. But not women, of course. 
 Tish also wanted to speak about the fact that she is a woman with five sisters, and that sexual offence statistics are
Tish also wanted to speak about the fact that she is a woman with five sisters, and that sexual offence statistics are 
 Some sports, like Rugby, did the right thing before the Supreme Court ruling. And others have done the right thing since. But even though sports governing bodies may adhere to the law, there are still clubs that completely ignore the governing bodies adherence. For example, British Rowing complied with the law ages ago. But it is only just in the last few days have Cambridge University complied.
Some sports, like Rugby, did the right thing before the Supreme Court ruling. And others have done the right thing since. But even though sports governing bodies may adhere to the law, there are still clubs that completely ignore the governing bodies adherence. For example, British Rowing complied with the law ages ago. But it is only just in the last few days have Cambridge University complied.


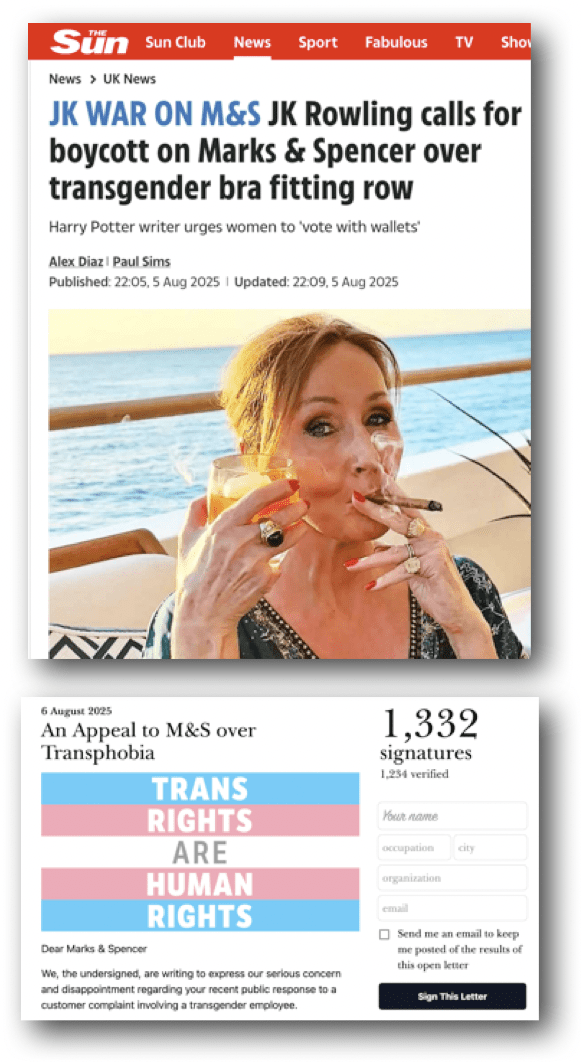
 On the 4th August, the Telegraph
On the 4th August, the Telegraph 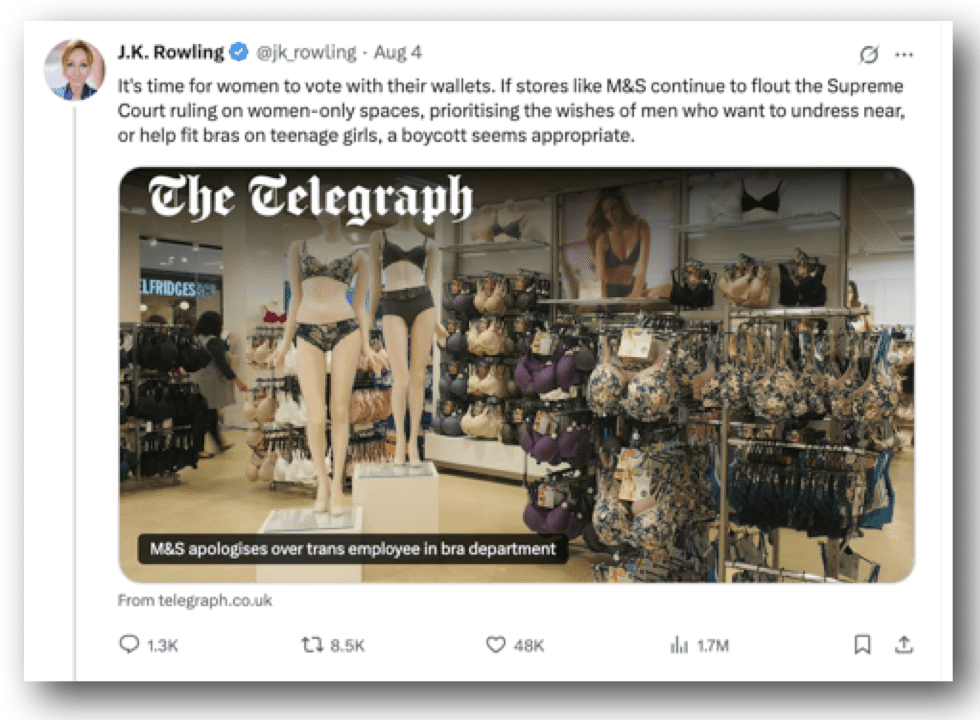
 “Show me a girl who is not self-conscious about her body at that age and I will show you a liar. It doesn’t matter how open you have been as a parent, it is all, as the kids say, “awks”,”
“Show me a girl who is not self-conscious about her body at that age and I will show you a liar. It doesn’t matter how open you have been as a parent, it is all, as the kids say, “awks”,” 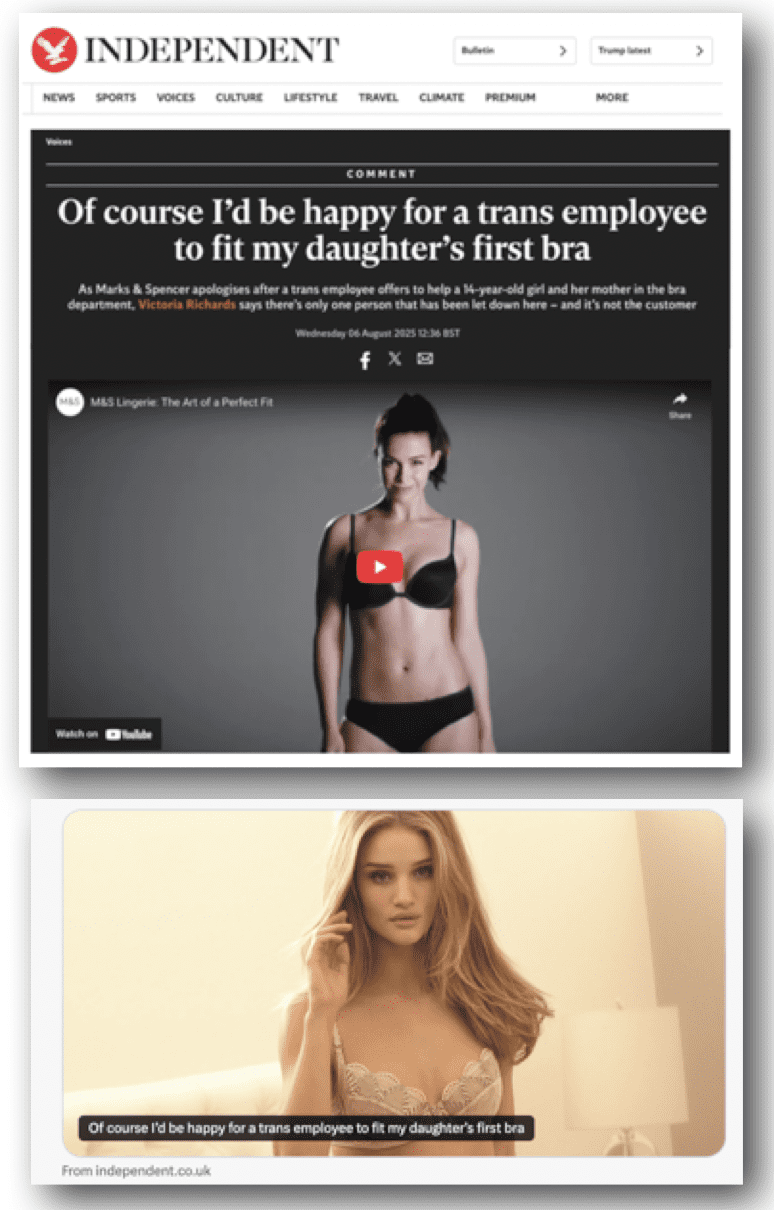
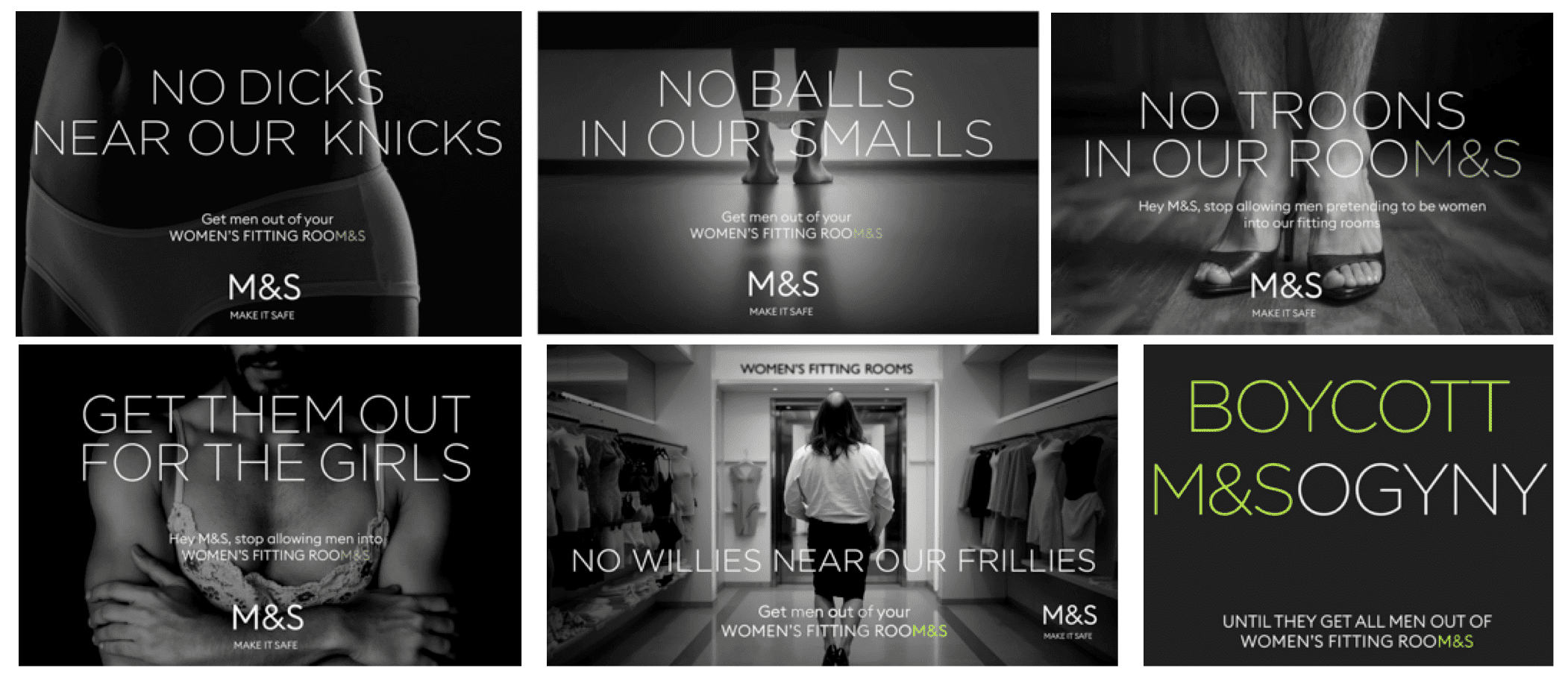

 Within a couple of days, one of the ‘Titter’ graphics had been made into a sticker by some enterprising women.
Within a couple of days, one of the ‘Titter’ graphics had been made into a sticker by some enterprising women. 

 Within days of opening the account, the girl’s mother had been accused of being a troll, a lying bastard, spreading hate, grifting, being a terrible parent and being a bigot (of course). Not just any old bigot but a stinking bigot, a fucking bigot, despicable, pathetic, hysterical, lying; cooking up bollocks, being attention seeking & over the top, and
Within days of opening the account, the girl’s mother had been accused of being a troll, a lying bastard, spreading hate, grifting, being a terrible parent and being a bigot (of course). Not just any old bigot but a stinking bigot, a fucking bigot, despicable, pathetic, hysterical, lying; cooking up bollocks, being attention seeking & over the top, and 

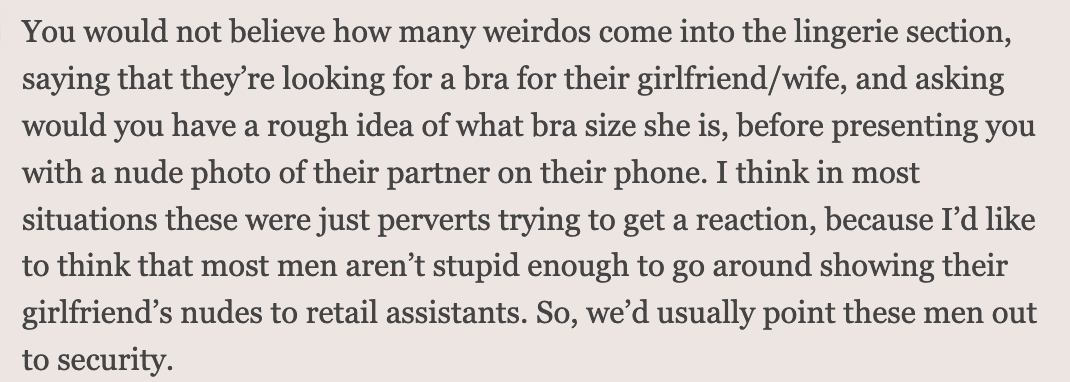 Lingerie shops are a magnet for male weirdos, the majority of whom are your gros, pervy straight guys. This is not news.
Lingerie shops are a magnet for male weirdos, the majority of whom are your gros, pervy straight guys. This is not news. 
 In 2020, the Telegaph ran a piece claiminng that M&S changing room policy could put girls at risk, after Baroness Nicholson wrote to the company expressing concerns.
In 2020, the Telegaph ran a piece claiminng that M&S changing room policy could put girls at risk, after Baroness Nicholson wrote to the company expressing concerns.