
The NHS was established in 1948, in the wake of the devastation of two world wars. The visualised dream of Sir William Beveridge, it was nurtured into being after the 1945 General Election, under the eye of Health Minister Aneurin “Nye” Bevan, the son of a coal miner, and Prime Minister Clement Attlee. In 1946 the National Health Service Act was published and in 1948 the NHS was created.
Funded by taxes and free at point of entry, it united medics, opticians, dentists and hospitals to provide a comprehensive National Health Service for the people of Britain. Originally, the idea met with a lot of opposition from the British Medical Council (BMC). Doctors were worried they would lose out financially. Bevan’s solution was to allow them to continue seeing private patients if they also accepted NHS patients, famously saying he had ‘stuffed their mouths with gold’ in order to get them to comply.
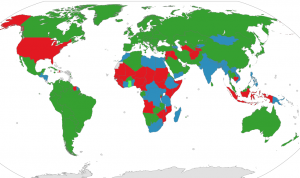
Countries in red have no free/universal healthcare
This all happened more than seventy years ago.
There are still over 40 countries in the world that have neither ‘free’ nor universal healthcare.
It’s hard for those of us who have never experienced life without an NHS to imagine what it was like for the average person before its creation.
The Sydney Herald, 12/4/50
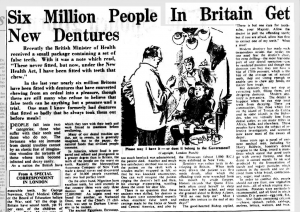
‘Saving up for the doctor’ was a very real budget consideration pre-NHS, for those that could even afford to consider it. Dental care was almost unheard of except among the wealthy.
In the first nine months of its existence the NHS created 33 million false teeth.
Just a few years later, in 1951, charges were brought in for dental and eye care and for prescriptions (one shilling), causing Bevan to resign from the cabinet in disgust.
In July 1959, the Mental Health Act brought the provision of mental health services within the administration of the NHS. In 2018, 1.44 million people were referred to NHS mental health therapy services.

Celebrating the Abortion Act
In 1961 the pill was launched, and its availability was extended to non-married women in 1967. In the same year the Abortion Act legalised abortion up to 28 weeks’ gestation for all women, not just if the life of the mother was in danger. This came into effect on 27 April 1968 (and was lowered to 24 weeks in 1990).
Although far from providing contraception or abortion ‘on demand’ these changes made an inconceivable difference to the lives and freedoms of British women.
The NHS must provide urgent treatment to anybody who needs it, regardless of whether or not they can pay for it. It is estimated that it loses somewhere between 15-25 million a year to ‘health tourists’ from abroad who use its services and don’t pay.

The first babies born on the NHS
NHS staff have delivered over 53 million babies since it was established in 1948. Born on the NHS? You can see what number baby you were by entering your birthdate here.
Our healthcare service is currently ranked 6th in the world (after Canada, Denmark, Sweden, Norway & Germany).
Sexism within the NHS
1950s postcard, England
The medical professions are no stranger to stereotyping: from the ‘sexy nurse’ to the all-knowing, hunky male doctor, it has been plagued as much as, if not more than, any other with stereotypes of gendered behaviour and misogyny.
In her 2019 article ‘Sexual Harassment in Healthcare‘ Susan Strauss observes:
“Florence Nightingale tried to control male physicians and surgeons’ sexual harassment of her nurses in the 1800s. Her approach was one of prevention – each nurse had to be of high moral character, thereby implying that nurses were to blame for their own victimization, which was the thinking of the time.”
Observing that sexual harassment is still rife in the medical profession, Strauss adds “studies vary as to who is the most likely perpetrator. Some research suggests it is the physician while others indicate it is the patient or relatives.”

The ‘fancy dress’ fantasy of the ‘sexy nurse’
“When I first started in the office older female colleagues told me to dress down because I had big boobs and would be an easy target.” reported Catherine Renton in an article titled ‘Sexual harassment is rife in the NHS – I know because I was subject to it for years’
“A Unison report titled ‘It’s Never OK’ reveals that the vast majority of those targeted (81%) were women,” continues the article in the Independent.
Visit the actual Unison report however, and the story is somewhat different. Unison inform us that ‘the vast majority (81%) of those harassed identified as female, and the rest (19%) male.’
And here the woowoo begins.
Nurses are not harassed because of their gender identity – nurses are harassed because of their sex.
A brief history of sexism in medicine
In Barbara Ehrenreich’s excellent pamphlet “Witches, Midwives, and Nurses” she writes:

JW Waterhouse ‘The Magic Circle’
“Women have always been healers. They were the unlicensed doctors and anatomists of western history. They were abortionists, nurses and counsellors. They were pharmacists, cultivating healing herbs and exchanging the secrets of their uses. They were midwives, travelling from home to home and village to village…. the great majority of them were lay healers serving the peasant population, and their suppression marks one of the opening struggles in the history of man’s suppression of women as healers. They were called ‘wise women’ by the people, witches or charlatans by the authorities… Witch-healers were often the only general medical practitioners for a people who had no doctors and no hospitals and who were bitterly afflicted with poverty and disease… We have not been passive bystanders in the history of medicine. The present system was born in and shaped by the competition between male and female healers. The medical profession in particular is not just another institution which happens to discriminate against us: It is a fortress designed and erected to exclude us.”
 ‘Higher education in women produces monstrous brains and puny bodies, abnormally active cerebration and abnormally weak digestion, flowing thought and constipated bowels’.
‘Higher education in women produces monstrous brains and puny bodies, abnormally active cerebration and abnormally weak digestion, flowing thought and constipated bowels’.
Dr E. H. Clark 1873
Women were not allowed entry into UK medical schools until the late nineteenth century. In 1881, there were only 25 women doctors in England and Wales. Thirty years later, this had risen to 495. Kings College Hospital and UCL began to train women in 1915. The first world war opened up positions in hospitals for women that would usually have been filled by men. In 1944 a government committee decided that funding would only be given to medical schools that accepted a reasonable proportion of women. This was set at ‘say around 1/5’ . In 1963, the Universities Central Council on Admissions recorded that women made up 34% of medical applicants and 29% of acceptances.
In 2002, 37% of practising medical doctors were women. Fast forward to 2020 and this has risen to 45%. In fact, women now outnumber men in British medical schools.
 So it would be easy to think that perhaps the battle for equality had been won…
So it would be easy to think that perhaps the battle for equality had been won…
An NHS careers study showed that 70% of children aged 7-11 picked a picture of a man when asked to identify a surgeon, and the same percentage picked a woman when asked to identify a children’s nurse.
Before we recoil in horror at the inner sexism of these youngsters, it should be noted that their estimations were optimistic – just 11% of consultant surgeons are women and just 11% of nurses are men.
 Perhaps such sexism is changing – in 2019, when one Twitter user posted this picture with the caption “This is cute, isn’t it?” many others pointed out the sexism in the presumption that the girl child would grow up to be a nurse and the boy a doctor.
Perhaps such sexism is changing – in 2019, when one Twitter user posted this picture with the caption “This is cute, isn’t it?” many others pointed out the sexism in the presumption that the girl child would grow up to be a nurse and the boy a doctor.
Many of the comments inferred the inferior nature of nursing as well as the stereotyping of the children, showing that nursing is valued less than ‘doctoring’.
Others spoke from personal experience.
“Ermm, no. No it is not (cute). It’s this sort of drip-feeding that has led my 4-yr old daughter to tell me girls can’t be doctors. Even tho her mother is a Doctor! Why do you insist on continuing these out-dated stereotypes?“ commented Dr Merryl Gelling.
“Why is everyone assuming they know the genders of these kids?” observed Dr Sapna Kudchadkar, but such is the confusion surrounding the meaning of the word ‘gender’ these days, I’m unsure if it was an observation on the sex of the kiddies- does long hair and a penchant for pink automatically mean ‘girl’?- or if she was referring to the mysterious inner gender identity that we’re all supposed to have these days.
Professor Mark Radford noted in ‘Nursing Times’ that even his own children have made comments such as “nursing is for girls” despite having a dad who is a nurse. Studies and reports suggest that stereotypes in nursing do not just harm female nurses but also men.
In 1951 the first male nurses joined the main nursing register. In 2004 the percentage of male nurses was 10.63%. This had increased to 10.69% in 2008, then to 11.4% in 2016.
“In the early 1950s, approximately 7% of general nurses were male. Today, nearly 70 years later, only 11% of all nurses are men.” reports the Royal College of Nursing.
Male nurses report frequently being asked if they are training to be doctors; colleagues and patients presuming they are gay, and that the job is often viewed as emasculating or demeaning, especially by other men. Because men are generally physically stronger than women, they are expected to restrain patients when necessary and expected to do more heavy lifting. Some studies suggest they experience higher rates of stress, anxiety and depression than female nurses, and they are more likely to leave the profession permanently.
However, men are often presumed to be in charge because of their sex, and men in nursing are over represented at higher pay grades, with men holding 27.5% of the best paid jobs at the top of the industry. This is almost certainly in part because more women take career breaks to birth (and raise) children. Because biology.
In 2018, almost 46% of all doctors on on the GMC register were women. This rose to 56% for those under 30.
This might be a good point to observe that if we continue to record ‘man’ and ‘woman’ in the gathering of data as a self-selected identity rather than a biological fact, collection of such date will be completely meaningless.
The concept of sex discrimination is, by its very definition, transphobic.
Despite this promising rise in women doctors, the sex pay gap – yes, the SEX pay gap, not the bloody gender pay gap- means male doctors earn 17 per cent more than their female counterparts. Women continue to be over-represented in the lower paid, less technically focused specialties. This is influenced by the fact that more women in the UK work part time. Again, one of the more obvious reasons for this is that if we want to have kids we are the ones who must break to birth the offspring.
Identify out of that.
‘The culture of the system does need to change… if you work less than full time you’re not taken as seriously – it’s known as the maternity penalty,’ reports Alex Matthews-King.
Biology Matters
 We need to be clear that the maternity penalty affects adult human females.
We need to be clear that the maternity penalty affects adult human females.
Let’s take a moment to state the obvious here, unfashionasble as it may be. Men do not have babies.
Misrepresenting the reality of sexism everywhere- and nowhere more than in the world of medicine – erases such realities.
It doesn’t matter in the least how we identify – nature has decreed that women are the ones that push those large-headed, big-eyed little humans out of our vaginas and into the world. In the world of medicine, our gender identities are meaningless.
Perhaps in no other field does the sex of our bodies hold such importance. Male is always the default.
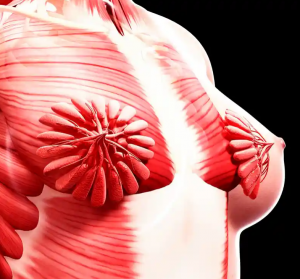
milk ducts
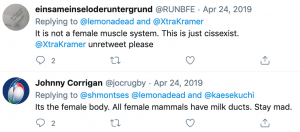
In 2019 a viral tweet (from a now suspended account) read, “I just realized I never saw a photo of a female muscle system. This is NOT what I imagined milk ducts to look like.”
“Woah, I must of learned what breasts look like by studying men’s breasts, cause this is BRAND NEW. I am thinking hard about patriarchy and our educational system,” observed a woman called Claudia. “I should not be this old and making discoveries about my own body over Twitter.”
Others were less impressed.
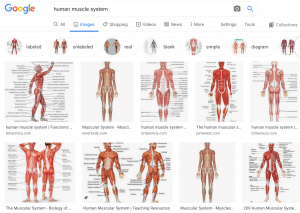
man is the human default: just ask Google
“Even without milk ducts, the scientific images of human bodies that we typically see have male builds and musculature. “ observed in the Guardian. “Troublingly, we don’t even necessarily identify them as male, and therefore specific only to half of the population. We see them as “normal”.
“Centuries of female exclusion has meant women’s diseases are often missed, misdiagnosed or remain a total mystery,” reports Gabrielle Jackson in the Guardian in 2019.
 Dr Kate Young notes: “In some of the first sketches of skeletons, male anatomy artists intentionally made women’s hips look wider and their craniums look much smaller as a way of saying: ‘Here is our evidence that women are reproductive bodies and they need to stay at home and we can’t risk making them infertile by making them too educated, look how tiny their heads are.’ And we see that again and again.”
Dr Kate Young notes: “In some of the first sketches of skeletons, male anatomy artists intentionally made women’s hips look wider and their craniums look much smaller as a way of saying: ‘Here is our evidence that women are reproductive bodies and they need to stay at home and we can’t risk making them infertile by making them too educated, look how tiny their heads are.’ And we see that again and again.”
Drug dosages, it has been revealed recently, are generally based on the requirements of male bodies. Between 1997-2000, 8 of the 10 drugs taken off the market posed more of a risk to women than to men.While doses are adjusted for weight, women’s bodies process certain medications differently.
Sex matters.
GRS on the NHS
1n 1999, a decision not to fund sex change treatment, now more commonly referred to as gender re-assignment surgery (GRS) on the NHS was found to be ‘operated as a blanket policy without proper regard for individual cases’ and declared unlawful. Thus gender reassignment surgery became a legal right on the NHS.
In that year, just 49 people had ‘the operation’. Ten years later, numbers had tripled, 80% of surgeries being performed on men who wished to become women. At the Charing Cross Clinic in London, the number of adult referrals almost quadrupled in the 10 years from 2007 (498) – 2016 (1,892).
Breast augmentation treatment for trans-identified patients is rarely provided on the NHS. In 2010, a trans-identified man challenged a decision by Berkshire West Primary Care Trust to refuse him breast augmentation treatment. The Trust had a policy which stated ‘GRS is a Low Priority treatment due to the limited evidence of clinical effectiveness and is not routinely funded.’ The court decided that there was ‘no general medical concensus to contradict the policy stance taken’.
It is estimated that less than 20% of people who identify as transgender undergo ‘bottom surgery’ GRS. Some undergo hormone treatments and some do not undergo either. Rising numbers of young women undergo elective double mastectomies. Waiting lists have soared to over 3 years in some areas. The BBC reports that over 13,500 transgender and non-binary adults are on waiting lists for consultations at NHS gender identity clinics in England.
The NHS no longer considers gender dysphoria to be a mental health condition, in line with the Diagnostic and Statistical Manual of Mental Disorders (2013).
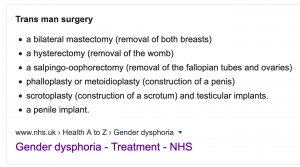
A quick Google shows that the NHS lists a variety of surgical procedures as treatment for gender dysphoria.

The NHS does not perform surgeries on young people under the age of 18.
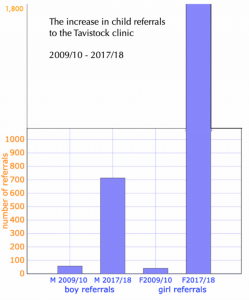
At the Tavistock and Portman NHS Foundation Trust, Britain’s primary children’s gender identity clinic, the number of referrals for under-18s has risen from 97 in 2009/10 to 678 in 2014-15, to 2,590 in 2018-19.
Regulatory Capture and training the NHS
In recent years many NHS trusts have been advised or trained by a variety of trans lobby groups such as Mermaids and GIRES.
The training of NHS service providers has led to some interesting changes in policy and in documentation.
The NHS Trusts in Nottingham released this spectacularly unscientific statement in their 2018 Trans Equality and Gender Reassignment Policy
“Research supports the belief that transsexuality is a condition developed by the foetus in the womb. At twelve weeks, if the foetus is to be male, the mother’s body produces a burst of the male hormone, testosterone, which masculinises the internal and external genitalia. However, it is not until four weeks later that a second hormonal trigger masculinises the brain of the foetus. Male and female brains differ significantly in the construction of the hypothalamus, which is responsible for the production of male/female hormones. Should one of these two hormonal triggers fail to occur, a baby will be born with the physical attributes of one gender, and the brain functions of the opposite gender.”
 This is astonishing nonsense: science has established no such thing. We do not have identifiable male and female brains nor does the release of testosterone perform such a specifically simplistic function as stated.
This is astonishing nonsense: science has established no such thing. We do not have identifiable male and female brains nor does the release of testosterone perform such a specifically simplistic function as stated.
Daphna Joel says, “the theory goes that once a fetus develops testicles, they secrete testosterone which masculinises the brain. If that were true, there would be two types of brain.” When her researchers looked at over 1400 brain scans they found that very few people had all of the brain features they would traditionally have been expected to have, based on their sex. Less than one person in ten had a ‘typically’ male or female brain. Most fell, predictably, somewhere inbetween.
Rice & Carothers 2014 study looked at over 100 different behavioural measures, and male and female scores could not be reliably (or accurately) grouped into two distinct categories. They concluded, ‘there is little support for believing that sex differences are anything more than individual differences that vary in magnitude from one attribute to another’.
Gina Ripon, author of ‘The Gendered Brain: The New Neuroscience That Shatters the Myth of the Female Brain‘ argues that despite social expectations of how boy and girl babies should behave, there ‘is nothing that reliably distinguishes brains of baby boys from brains of baby girls’. Men, on average do have brains 10% bigger than women but they also have bigger kidneys and ‘nobody suggests we have gendered kidneys’.
Nor has anyone suggested that trans-identified men have smaller brains than other men.
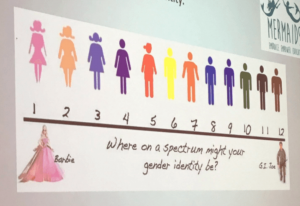
Are you GI Joe or Barbie?
So why are NHS Trusts releasing statements like the one above?
Mermaids, who infamously trained UK police officers using the ‘GI Joe to Barbie’ gender spectrum scale, are notorious for promoting unsubstantiated ideas which promote regressive gender stereotyping. Mermaids receive hundreds of thousands of pounds in funding from organisations like The National Lottery, and spend much of it providing ‘trans-inclusive diversity awareness training‘ to police forces, social services, schools and the NHS.
 At a 2015 NHS Symposium (link to minutes) attended by both GIRES and Mermaids, speakers- including one who described having a gender identity ‘in flux’ and ‘constantly evolving’- told attendees that the valuing of ‘real life experiences’ in NHS assessments was ‘cruel and unnecessary… dangerous and it kills people’. Another speaker accused NHS clinicians of ‘manipulative gatekeeping’.
At a 2015 NHS Symposium (link to minutes) attended by both GIRES and Mermaids, speakers- including one who described having a gender identity ‘in flux’ and ‘constantly evolving’- told attendees that the valuing of ‘real life experiences’ in NHS assessments was ‘cruel and unnecessary… dangerous and it kills people’. Another speaker accused NHS clinicians of ‘manipulative gatekeeping’.
A third was happier, having got an appointment within just 3 months and waited less than 18 weeks for surgery.

Birmingham’s NHS Foundation Trust ‘trans and non-binary policy has this to say:
“If, in an emergency situation, it is unclear if the patient is Trans (because they are unconscious) the staff need to try and ascertain the person’s preferred gender before contacting the family or moving to a ward. For example, the staff may look for forms of identification the patient has to see if this will indicate their preferred gender.”
Yup, they are seriously suggesting that staff should rummage through belongings, looking for ID, in an attempt to find out the gender identity of an unconscious patient before contacting their family- you might use the wrong pronouns!- or moving them to a single-sex ward – a male-bodied person might have wanted to be on a woman’s ward!
The document also states: “The patient must be in a same-sex environment of their preferred gender.”
What does that even mean???
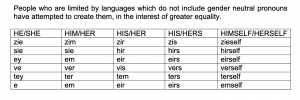
The resource ends in a lament about the inadequacy of the English language when describing non-binary identities and a quick lesson on pronoun usage.
In 2017, All About Trans, Gendered Intelligence, the Proud Trust and Mermaids, including at least one trans-identified child, met with NHS England staff to discuss how the NHS could ‘improve’ and be ‘more trans inclusive’. The interaction began with an introduction and sharing of pronouns. Criticism included trans patients being correctly sexed and having their legal names used on documentation.
NHS England published a consultation on gender identity services in 2017 after GPs complained that they did not have ‘the proper expertise‘ to provide prescriptions for hormones to trans-identified people.
Mermaids is not the only trans lobby group providing ‘training’ to medical professionals. In 2019 an online GIRES trans training course for doctors was scrapped by the Royal College of General Practitioners (RCGP) after GPs claimed it led to ‘unrealistic expectations’ and pushed them towards recommending surgery to patients. There were also objections to the promotion of Mermaids, who the RCGP called ‘very controversial’.
Other NHS-sponsored online courses remain.
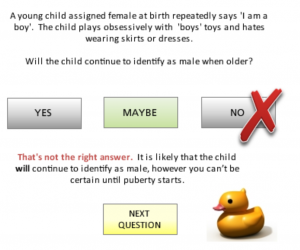 “The Gender Variance e-learning programme is designed for healthcare staff of all levels and disciplines.”
“The Gender Variance e-learning programme is designed for healthcare staff of all levels and disciplines.”
It is produced by GIRES and funded by NHS Health Education Kent, Surrey & Sussex.
The course asserts several times that that once puberty starts you can be certain whether a child is trans or not, in one case stating that a teenage girl calling herself Jack, who is distressed by puberty and doesn’t like going out ‘has reached puberty which means his feelings will be unlikely to change’.
After completing the course participants are able to sit a multiple choice test. Those who obtain 80% or above are entitled to a ‘Continuing Professional Development Test’ certificate. This certificate can be printed out by professionals and displayed in their office.
Yay!
Go me.
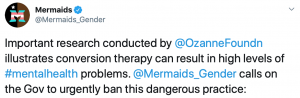
Despite the spiraling costs, long waiting lists and rising numbers of detransitioners, the NHS no longer appears to advise that some people might benefit from psychological help coming to terms with their sexed bodies. Would that be so very terrible? Well, probably. Anything other than immediate and total affirmation of a trans identity is now erroneously referred to as ‘conversion therapy’ by lobby groups such as Mermaids, who never tire of suggesting that the mere discussion of such a possibility leads to worsening mental heath problems and even encourages trans-identified people to kill themselves.
While Mermaids isn’t mentioned on the Tavistock website it is featured in the NHS guides ‘A Guide for Young Trans People in the UK’ and ‘A practical guide for the NHS’ as a support and information organisation.
It’s not about the money
In 2015, ITV reported that “the cost of gender reassignment is £19,236 per patient, including support as well as surgery. The total cost to the NHS in England last year was £17.13 million and this year the budget has been increased to £22.72 million.”
This sounds a lot, but in the great scheme of things, it isn’t. In fact, it’s just 0.02% of the overall NHS budget for 2015, which was £102 billion.
In theory the NHS will only carry out a cosmetic procedure if there is a ‘clear clinical need’ and if someone’s physical and mental health could be at risk without it.
In 2014 a survey by a firm of medical negligence solicitors found that one in four patients undergoing cosmetic surgery procedures including rhinoplasty, breast enlargement and facelifts had lied to secure NHS funding, claiming depression or other mental health issues as a result of their appearance.
In the same year liposuction alone cost the NHS an astonishing £9.6 million. Even if the ‘gender reassignment’ budget had doubled since 2015 (which it hasn’t) it would still only be 0.03% of the current NHS budget of £152.9 billion.
So it really isn’t about the money. Recovery times, complications, painful scar tissue, we should all be able to agree that nobody should be suggesting that transition is an easy option.
Enter the NHS.
Watch your language
 It is about the language.
It is about the language.
‘Gender reassignment’?
Who assigns a gender? A god? Other humans? The gender fairy?
Somebody has to do the assigning.
And what exactly is gender? And if we aren’t even sure about that, how can it possibly be reassigned? An operation can change a body. It can’t ‘reassign a gender’.
So where does the NHS stand in all this? Are proper precautions being taken to protect those who believe themselves to be something they aren’t?
Living my Life
Which brings us to the glossy-paged joy of ‘Living My Life’.
Type ‘NHS transgender’ into Google, & one link will be to a 25 page brochure called ‘Living my Life’.
 If you are, or think you might be,“bi-gender, transgender, FTM, transwoman, MTF, transman, third gender, transvestite, crossdresser or transexual” this is the document for you.
If you are, or think you might be,“bi-gender, transgender, FTM, transwoman, MTF, transman, third gender, transvestite, crossdresser or transexual” this is the document for you.
The brochure is described as offering ‘information for people who currently identify as trans or who are beginning to explore their gender identity’. Paper copies are available from www.sexualhealthsheffield.nhs.uk
And that’s pretty interesting, right? After all, we’re frequently told these days that we all have a gender identity, so it makes sense that anyone confused about theirs – or wondering where it is – might expect to find helpful and clarifying information inside the pages of this brochure.

Pictures from ‘Living my Life’
Inside, models represent a teenage girl thanking her mum for supporting her in her quest to be a boy, and an older man who is as keen that the world should see his enormous breasts as the young woman is that the world should forget about hers.
Scroll further down and you’ll see Aimee Challoner and friend, two trans-identified men, all highlights and lip gloss, tip their glasses ‘sexy secretary’ style and wink at the camera.

The brochure tells readers: “A transgender person is someone whose personal idea of their gender does not match with his or her assigned gender role.”
Now while society certainly has expectations about the way men and women should behave, we do not live in a country where we are literally assigned gender roles.
We do not have a gender police patrolling the streets to ensure that everyone is correctly performing the gender role excepted of them – although that’s a short story I’ve been meaning to write for some time now.
Nowhere does the brochure suggest what these roles are but we can assume – for assume the reader must – that ‘assigned gender roles‘ are such stereotypes as cool young men in beanies who form rock bands and women who become belipsticked sexy secretaries. And this is, for want of a better phrase, sexist nonsense and the NHS should know better.
“The word trans is useful as an ‘umbrella’ word. It is generic and captures the variety of trans identities without being limiting,” continues the brochure, helpfully. “Many services and organisations now use trans to refer to anyone who crosses traditional gender boundaries – whether permanently or periodically. (my emphasis)”
This seems to be genuinely suggesting that if I put up a shelf, a typically ‘manly’ task, then I’m ‘crossing traditional gender boundaries and am temporarily transgender. This muddled thinking is not helpful to anybody. By this definition there are probably very few of us who aren’t transgender, which is obviously absurd.
 The confusion is further compounded by the brochure’s definition of ‘Gender Queer’. A person who is Gender Queer may identify as genderless. Or Agender.
The confusion is further compounded by the brochure’s definition of ‘Gender Queer’. A person who is Gender Queer may identify as genderless. Or Agender.
This brochure is NHS recommended. Our good old solid, dependable NHS.
FFS, if anyone should know about Biology, they should.
Desistence & detransition
But at the same time as more and more people are coming forward wanting to medically transition, we are also experiencing a backlash from those, like Keira Bell, who feel that body modification treatment shouldn’t have been so easily available.
Bell says the feeling of needing to ‘change her gender’ built up the more she read about it online. In March 2020 it was reported that she was taking legal action against the Tavistock and Portman NHS Trust ‘for not challenging decisions about transition that she made as a teenager’.
 “I should have been challenged on the proposals or the claims that I was making for myself, and I think that would have made a big difference as well, if I was just challenged on the things I was saying… I was allowed to run with this idea that I had, almost like a fantasy, as a teenager…. I’m very young. I’ve only just stepped into adulthood…. at the time I felt it relieved all those mental health issues I was feeling, alongside gender dysphoria… I feel I could say anything to my 16-year-old self and I might not necessarily listen at that time. And that’s the point of this case, when you are that young you don’t really want to listen.”
“I should have been challenged on the proposals or the claims that I was making for myself, and I think that would have made a big difference as well, if I was just challenged on the things I was saying… I was allowed to run with this idea that I had, almost like a fantasy, as a teenager…. I’m very young. I’ve only just stepped into adulthood…. at the time I felt it relieved all those mental health issues I was feeling, alongside gender dysphoria… I feel I could say anything to my 16-year-old self and I might not necessarily listen at that time. And that’s the point of this case, when you are that young you don’t really want to listen.”
Jacob
 In 2019, 16 year old Jacob, a girl who felt ‘weak and inferior to men‘ before deciding to transition, reported to The Times that taking puberty blockers on the NHS was “the worst decision I’ve ever made,” and claiming puberty blockers had been “sold to me as a miracle cure for being trans.”
In 2019, 16 year old Jacob, a girl who felt ‘weak and inferior to men‘ before deciding to transition, reported to The Times that taking puberty blockers on the NHS was “the worst decision I’ve ever made,” and claiming puberty blockers had been “sold to me as a miracle cure for being trans.”
In the same year the Royal College of Paediatrics and Child Health asked its committee of experts to “look at the ethics around the rapid increase in the use of hormone blockers to treat under-16s who identify as transgender”.
Jacob claims negative effects of taking the blockers included depression, insomnia, exhaustion, fatigue, low moods, rapid weight gain and a reduction in bone density which resulted in four broken bones.
“They (GIDS) asked a 12-year-old to make a decision an adult would struggle with… it was like, ‘here are the drugs’ and off we went… my Tavistock worker was saying to me, ‘once you have the testosterone, you’ll be a boy… if anything, I’ve been more depressed than before.”
These cases are not isolated.

Men and women in hospital wards
In 2010 Andrew Lansley (then Health Secretary) said: “”Patients should not suffer the indignity of being cared for in mixed sex accommodation.”
A scheme was brought in whereby NHS hospitals had to pay a fine of £250 per day for keeping patients on mixed-sex wards. A year later the BBC reported that single-sex wards were now ‘the norm’ and Lansley was quoted as saying, “The NHS has done a fantastic job getting to grips with this. Single-sex accommodation is what people can now expect.”
With the rise of the influence of gender identity such pledges and regulations have become entirely meaningless. An NHS that believes that gender identity is ‘assigned at birth‘ and that people can be ‘born in the wrong body’ is inevitably going to get into hot water when it tries to balance these two very different objectives.
Case 1
 In 2016, Phillipa Molloy was admitted to a secure psychiatric hospital suffering from a condition that left her terrified of men, including her own husband.
In 2016, Phillipa Molloy was admitted to a secure psychiatric hospital suffering from a condition that left her terrified of men, including her own husband.
“Because of that,” she reports, “I was taken and placed in a female-only unit.”
When a trans-identified man was put on her all-female ward, where he wandered around in a short dressing gown, she says she was left “genuinely, absolutely terrified”.
A spokesman for Lancashire Care NHS Foundation Trust claimed it had been following Equality Act guidelines and that legal advice had directed them that “transgender people should be able to self-identify and receive treatment on the ward that is appropriate and in line with that self-identification.“
Case 2
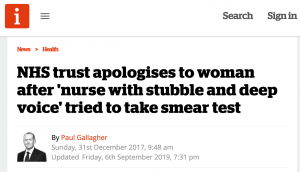 In 2017 an NHS Trust apologised to a woman who had specifically requested a female nurse for her smear test after a bearded man appeared and told her “My gender is not male. I’m transexual.“
In 2017 an NHS Trust apologised to a woman who had specifically requested a female nurse for her smear test after a bearded man appeared and told her “My gender is not male. I’m transexual.“
The patient asked to remain anonymous because she didn’t want the clinic or the nurse to be criticised.
“[It was] weird,” she told The Sunday Times, “where somebody says to you: ‘My gender is not male’ and you think: ‘Well, what does that even mean? You are clearly a man.”
What does that even mean?
 In 2019 Joani Walsh reported that as a result of a clause in the DoH guidance, “a physically intact male has the right to choose to be treated on a ward for women that is simultaneously declared to be single sex.”
In 2019 Joani Walsh reported that as a result of a clause in the DoH guidance, “a physically intact male has the right to choose to be treated on a ward for women that is simultaneously declared to be single sex.”
More than 80 per cent of people who identify as transgender don’t undergo ‘gender reassignment’ surgery, yet they can be registered to stay on the sexed ward of their choice by evoking ‘gender identity’. As NHS data systems record patients as their preferred choice of sex, exact numbers can’t be measured, but multiple cases have occurred.
West Suffolk NHS Trust even asserted the right of a trans-identified patient over the right of other patients to single-sex space, claiming it “supersedes objections raised by other patients”.
The Telegraph newspaper was contacted by a nurse who reported that “a well-built, tall patient who had breast implants but intact male genitalia” appeared sexually aroused on a female ward, rubbing his penis through his night clothes and ‘causing distress to other patients’.
This confusion surrounding sexed bodies is further compounded by the NHS and government acceptance of the concept of non-binary people, who evidently belong to neither sex. The inability of the health service to clearly define the difference between sex and gender leads to genuine problems.
“For non-binary people, there is no appropriate single-sex ward for us. Whether we are in a male or a female ward, we will be misgendered,” laments Charlie in Mental Health Today, who believes that some non-binary identified women have ‘presentations too masculine for women’s spaces’.

We are left, for want of a better phrase, with a right bloody mess.
The issue in medicine, in health, is concern for our bodies. All bodies are different, but there are specific difference between men and women’s bodies that cannot be ignored. The issue is biology. Men and women have different bodies. That does not deny the existence of intersex people, in the same way that the existence of blind people is not denied when we describe humanity as a ‘sighted species’. There is a biological binary within the human species. It is unscientific to suggest otherwise. Humans reproduce via sperm and ova. Sex is not a spectrum.
The rest is personality. A rainbow of identities, cultural, personal, political, sexual. These identities are as personal as they are diverse. We humans are a jigsaw, made up of millions of tiny complexities, and the way we view our position within our society’s cultural expectations of gendered behaviour is a part of who we are. But it does not, nor can it ever, change our sex.
Sex chromosomes were discovered in 1905 by a geneticist called Nettie Stevens. Project Nettie, founded in her name, expresses its concern that “in contradiction of evolutionary history and millennia of human observations, highly-esteemed scientific periodicals are running articles undermining the observable reality of biological sex.”
“Biological sex is fundamentally defined by male and female reproductive anatomy. Attempts to recast biological sex as a social construct, which then becomes a matter of chosen individual identity, are wholly ideological, scientifically inaccurate and socially irresponsible.”
You can read the full statement here, where verifiable scientists are also able to add their signatures to the growing list of Project Nettie supporters.
Let’s revisit the ‘Living my Life’ brochure.
 Scrolling past a picture of a person with a large guitar and a partial buzzcut (Frank) who assures the reader ‘it does get better’, I’m tempted to wonder where the proof of that is.
Scrolling past a picture of a person with a large guitar and a partial buzzcut (Frank) who assures the reader ‘it does get better’, I’m tempted to wonder where the proof of that is.
There have been at least three studies (discussed here) which infer that suicide rates may even increase post-transition, especially in trans-identified men.
Instead of attempting to reassure the reader that there are other options to medical transition, the brochure seems to merely expand the bandwidth of what it means to be ‘trans’ even further.
Questions it’s suggested the reader might ask themselves include:
‘Although my external appearance might be that of a male/female– is this really how I feel?’
What isn’t clarified, of course, is what ‘feeling’ like a male or a female would entail. Do you really feel like a man or a woman is supposed to feel? Do you really? How would you know?
The curious reader is informed that trans may even include ‘not transitioning but occasionally wearing clothes usually associated with the ‘opposite’ gender’ or ‘being gender neutral and not wishing to present as either male or female.’
 What are we to make of this? Do those descriptions not describe the majority of us?
What are we to make of this? Do those descriptions not describe the majority of us?
Don’t we all want to control how we look and do what we want to do?
What message does this give to a young person (or even a not-so-young person) who is already feeling ‘othered’ by society and unsure where or how to find their place in the world? Could it be that those weird, awkward feelings are actually because they’ve been born in the wrong body?
Could medical transition actually fix it all?
“It is important to acknowledge that not all trans people are able to or choose to have genital corrective (or reassignment) surgery. For others, however, this is an incredibly important stage in correcting the gender they were assigned with at birth and in living the life they want to live.”
While the above paragraph initially reads as if it is intended to be objective, a quick look at the language used shows it’s anything but. The repetition of the concept of being ‘correct’ as opposed to being ‘wrong’; the idea that some unfortunates are ‘unable’ to benefit from this ‘incredibly important stage’ combined with the tantalising promise of ‘living the life (you) want to live’ – what’s not to like? After all, who wants to be assigned a role in life when you can choose your own?
The paragraph has been carefully worded to leave little question in the reader’s mind that transition is a desirable and attainable state of affairs. We’ve travelled so far down the misrepresentation highway at this point that it become almost impossible to unpack the multitudinous twists and turns of the language being used.
The only certain thing you can take from the brochure so far is that if you weren’t confused when you started reading it, you almost certainly are now. But this is ‘official’ stuff, right? This isn’t just some woowoo on the internet, this is a link directly from the NHS website.
 Wide-eyed Alex-Scott, who TBH looks about twelve, tells us, “At first you are not quite sure exactly who you are; but you learn. Then, society is not quite sure who you are; but eventually that changes too.”
Wide-eyed Alex-Scott, who TBH looks about twelve, tells us, “At first you are not quite sure exactly who you are; but you learn. Then, society is not quite sure who you are; but eventually that changes too.”
All this change and acceptance sounds wonderful, but nowhere on the NHS website are there pictures telling teenage girls they should be accepted just as they are, or telling middle-aged men that there’s more to being a woman than flashing your tits.
Nor was I able to find anywhere where the NHS suggests counselling may help to resolve these feelings, or acknowledging that for some people gender dysphoria goes away, while many others learn to live with it.
The brochure is very clear about one thing. Thinking you are something you’re not is NOT to be considered a mental health issue in itself. Trans health issues may include “mental health issues that have their roots in experiences of discrimination and transphobia” but these are a result of hatred and discrimination, not a confused mind. It is also important to remember that “some trans people experience mental ill health that is completely separate from their gender identity and should be treated as such.”
In among a long list of potential surgeries available on the NHS there are a long list of inane platitudes more suited to posters on a 13 year old’s bedroom wall.
What kind of medical health site tells people ‘we’re here for a good time not a long time’?
Pass the crack pipe and the vodka bottle, WTF, eh, YOLO.

Still not sure?
Well, ‘the first person to come out to is yourself’.
Still not sure?
‘Try to act confidently even if you don’t feel confident.’
Still not sure? Don’t worry, you’re fixable.
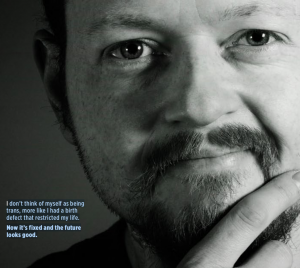 “I don’t think of myself as being trans,” pontificates Rob. “More like I had a birth defect that restricted my life. Now it’s fixed and the future looks good.”
“I don’t think of myself as being trans,” pontificates Rob. “More like I had a birth defect that restricted my life. Now it’s fixed and the future looks good.”
Still not sure?
Links to Mermaids and GIRES should help sort you out.
A change of tune?
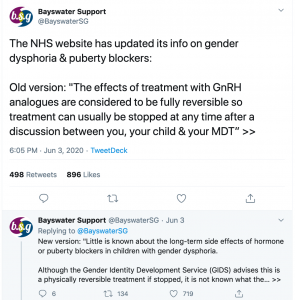
Until just a few weeks ago, advice on the NHS gender dysphoria page read, ‘The effects of treatment with GnRH analogues are considered to be fully reversible, so treatment can usually be stopped at any time…’
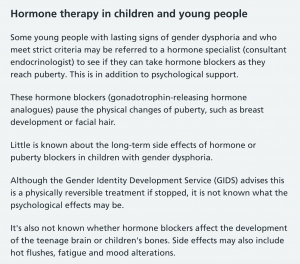
This week it was noticed that it has been quietly changed, after the last review on May 28th, to the far more cautious:
This turnaround caused James Kirkup to ask in this week’s Spectator:
“Given that the NHS now says that hormone therapy for gender-variant children has unknown long-term effects on the physical and mental health of those children, why is the NHS still using such treatments on children?”
Indeed. Many websites, including Northern Ireland group ‘Well’ are still currently promoting the old guidelines:
Mermaids still claims that puberty blockers ‘simply’ give a child time to reflect:
and a Mermaids factsheet for health professionals still advises: “puberty blockers (are) completely reversible and just suppresses the natural hormones for a while, giving time for further assessment and a chance for the child to learn whether they like being without their natural hormones or not.”
Will they be changing this advice?
 The Times reported, back in 2109, that Mermaids was giving advice that was ‘misleading and dangerous’ to attendees at training sessions, claiming that puberty blockers were ‘completely reversible’ and should be freely prescribed to children as young as 12.
The Times reported, back in 2109, that Mermaids was giving advice that was ‘misleading and dangerous’ to attendees at training sessions, claiming that puberty blockers were ‘completely reversible’ and should be freely prescribed to children as young as 12.
 More recently, in January 2020, the Guardian reported on the case involving ‘Mrs A’, the mother of an autistic girl being treated by GIDS who was bringing an action against the NHS. Her barrister, Jeremy Hyam QC, spoke of the ‘serious and life-changing’ consequences of prescribing “puberty-suppressing hormone blockers and then subsequently cross-sex hormones to children under the age of 18.”
More recently, in January 2020, the Guardian reported on the case involving ‘Mrs A’, the mother of an autistic girl being treated by GIDS who was bringing an action against the NHS. Her barrister, Jeremy Hyam QC, spoke of the ‘serious and life-changing’ consequences of prescribing “puberty-suppressing hormone blockers and then subsequently cross-sex hormones to children under the age of 18.”
It seems safe to assume that changes to the NHS web page giving advice on puberty blockers has been inspired by this turn of events.
Which leads me to ask, will the NHS be disassociating themselves from a brochure which not only glamourises transition but glorifies a life cut short with the line ‘we’re here for a good time, not a long time’?
YOLO, right?
Thank you for this exhaustive analysis of the insanity of gender ideology as it manifests itself in the medical system. It is truly surreal to be watching this unfold.
This is a real eye opener. Especially the request that female breast tissue pictures be taken down (!)and the misinformation under the umbrella of the NHS. A great read.
Wow, this is an amazingly informative article from someone who can smell the coffee – as an older woman I am fearful of a looming dystopia, but work like this gives me hope – thank you Lily.
Fascinating piece of work Lily! As another older woman I’ve watched most of the changes to the NHS documented here. I can attest to disbelief, dismay and discomfort in finding myself, at 60 years old, drowsy, tired and emotional after several hours in A&E, admitted in the early hours of the morning to a medical assessment ward peopled almost entirely by men. I can also attest to suffering unexpected side effects from being treated with various blood pressure lowering medications normally used in males. Here, there is a parallel with the untested and regulated hormone treatment of minors. I was prescribed a drug to lower blood pressure called doxazosin and found myself suddenly suffering stress incontinence. On investigation I discovered this drug had initially been developed to relax the urethra in men with prostate problems and was the subject of a class action in the USA by women who, having been prescribed it, developed urinary incontinence and underwent unnecessary surgery to correct it. I have shared this article, it deserves wide circulation. Thank you Lily.