 Those pesky dinosaurs, hoarding their rights all over the place! Dinosaurs, cervixes, women’s rights, trans rights, secret hoards of rights, bodies with vaginas, is there a pie or is there not a pie?
Those pesky dinosaurs, hoarding their rights all over the place! Dinosaurs, cervixes, women’s rights, trans rights, secret hoards of rights, bodies with vaginas, is there a pie or is there not a pie?
 There have been some pressing questions in the last few weeks as the levels of absurdity rise ever higher in humanity’s ongoing attempt to deny the biological sex exists: or at least that if one must accept that it does exist, to deny that it is any longer of any significance once washed in the bright and pure light of gender identity.
There have been some pressing questions in the last few weeks as the levels of absurdity rise ever higher in humanity’s ongoing attempt to deny the biological sex exists: or at least that if one must accept that it does exist, to deny that it is any longer of any significance once washed in the bright and pure light of gender identity.
Want to skip the background? Scroll down to the protest…
Lammy ask you about that…
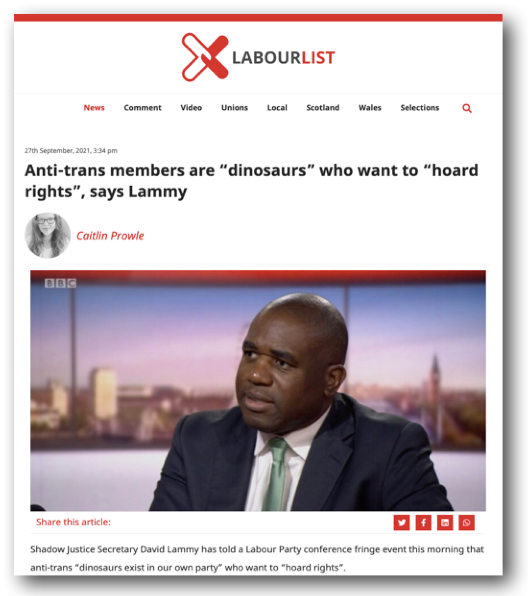 MP and Shadow Justice Secretary David Lammy sparked controversy late last month when he told a Labour Party Conference fringe event that women concerned with the preservation of single-sex spaces were dinosaurs guilty of attempting to hoard rights.
MP and Shadow Justice Secretary David Lammy sparked controversy late last month when he told a Labour Party Conference fringe event that women concerned with the preservation of single-sex spaces were dinosaurs guilty of attempting to hoard rights.
Fellow MP Joanna Cherry tweeted, “I’m very disappointed in you @DavidLammy. I’m not a dinosaur hoarding rights. I’m a woman & a lesbian whose life & professional experience as a sex crimes prosecutor has taught me why women & girls need the sex-based rights your party’s #EqualityAct guarantees”.
Lammy’s comments left women on social media both intrigued and incensed.
“I can’t think of any context in which “hoarding rights” is a sensible or useful construct,” observed mumsnet user allmywhat.
“You can’t hoard rights,” responded PlanDeRaccordement, adding, “and dinosaurs are extinct, is he saying women are extinct?”
“This is a slightly different hymnsheet to usual,” noted NecessaryScene, “and possibly more honest. Normally it’s ‘rights are not a pie’ and an insistence that no rights are being taken away.”
Lammy’s speech, which I’ve still been unable to track down in its full glory, referred to ‘anti-trans members’ of the Labour Party, rather than specifically referring to or naming women, although of course the recent demonisation of Rosie Dufflield may spring to mind (more on that later).
He later made a half-hearted attempt to clarify his statement, claiming that unless somebody specifically identified as ‘anti-trans’ it wasn’t them he was referring to as a rights-hoarding dinosaur.
So that’s all fine then.
what does ‘anti-trans’ mean?
Despite the serious and potentially devastating implications of the accusation, the label ‘anti-trans’ is vague and ill-defined.
 One thing we do know is that accusations of ‘anti-trans-ness’, more commonly known as ‘transphobia’, have resulted in the most terrible bullying of women, some of whom have lost their jobs and professional reputation for saying things that most of the population would consider completely reasonable.
One thing we do know is that accusations of ‘anti-trans-ness’, more commonly known as ‘transphobia’, have resulted in the most terrible bullying of women, some of whom have lost their jobs and professional reputation for saying things that most of the population would consider completely reasonable.
So we now know Lammy was only talking to the self-identifed ‘anti-trans’ it follows that anyone who objects to what he said is, ergo, an evil transphobe. Neat.
Nick Ferrari on LBC asked Lammy, “is it transphobic to say ‘only women can have a cervix’?”
“I don’t know if it’s transphobic,” mused Lammy, “but it’s not accurate, Nick. Obviously you- it’s probably the case that transwomen don’t have ovaries… but a cervix, I understand, is something that you can have following various procedures and hormone treatment and all the rest of it.”
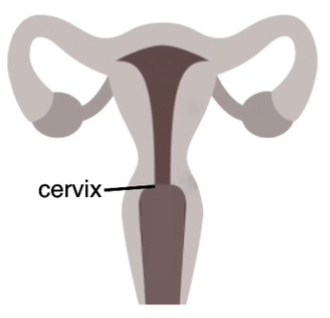 This is, of course, complete bloody nonsense. A cervix is ‘a cylinder-shaped neck of tissue that connects the vagina and uterus’. An inverted penis, or sheath made of other body tissue is not going to come with a cervix thrown in for good measure. Why would it? No bloke is going to be checking he’s 9cm dilated before starting to push out a baby- why would he need a cervix with his neovagina?
This is, of course, complete bloody nonsense. A cervix is ‘a cylinder-shaped neck of tissue that connects the vagina and uterus’. An inverted penis, or sheath made of other body tissue is not going to come with a cervix thrown in for good measure. Why would it? No bloke is going to be checking he’s 9cm dilated before starting to push out a baby- why would he need a cervix with his neovagina?
There are a small number of trans-identified men (TIM) who fetishise the idea of their own pregnancy. Some have joined breastfeeding groups on Facebook. Pregnant sissy porn is ‘a thing’. But in reality we are still many years from even attempting to transplant a full reproductive system into a man. Nonetheless, earlier this year Berkeley prof Grace Lavery joyously speculated that the day would soon come, tweeting pensively, “Just realized: someone alive today will become the first trans woman to get an abortion. <3″
To return to the point: it’s disconcerting that an elected representative of the people would let such utter blither pour out of his mouth and then make no attempt to refute it.
 It’s also interesting to note that Lammy only sees the dialogue from the perspective of trans-identified men, not trans-identified women. Rather than realising that ‘only women have cervixes’ is ostensibly transphobic because some of those women identify as men, Lammy views it from the male perspective: considering it easier to contemplate the possibility that a man has actually had a cervix constructed or transplanted into his body.
It’s also interesting to note that Lammy only sees the dialogue from the perspective of trans-identified men, not trans-identified women. Rather than realising that ‘only women have cervixes’ is ostensibly transphobic because some of those women identify as men, Lammy views it from the male perspective: considering it easier to contemplate the possibility that a man has actually had a cervix constructed or transplanted into his body.
On the Today program Lammy again dodged questions surrounding his speech, and told Nick Robinson the issue of how ‘trans rights’ affects women’s rights had ‘never come up on the doorstep’. This is a statement which some of his constituents deny.
“You said there are dinosaurs that exist in our own party that want to hoard rights.” asserted Nick Robinson.
‘I will always stand with those from a minority community,’ replied Lammy, immediately and irrelevantly.
When Rachel Burdon asked him, on Radio 5, “is it transphobic to hold the position that women born biologically female are entitled to their own spaces? Is it transphobic to hold that position?” Lammy responded by saying he didn’t want to ‘pour petrol on the fire’.
“Well maybe you shouldn’t use the word dinosaur and talk about hoarding rights as if rights are some kind of pie with a finite end,” retorted Rachel, who deserves a bloody medal.
“I’m someone who identifies as a feminist so I’m not going to take lectures on rights,” blustered Lammy. The irony of a man who calls himself a feminist talking over the top of a woman trying to talk about her rights appears to have been somehow lost on him.
Why pick on poor old David, some have asked? He seems like a nice bloke with good intentions. I’ve heard that he gets a lot of racist abuse, which is sickening. His work surrounding class and racism is admirable. As politicians go, he’s almost certainly one of the better ones. I know a woman who knows his wife. She pointed out that Nicola Lammy probably isn’t enjoying this much either.
My answer to the ‘why’ question is that there is a time to ‘be nice’ and a time to, well, not be so nice.
Politicians are our elected representatives. As such, they need to be careful with their words. Lammy may have thought he was being kind and inclusive, but at what cost? To the extent that he called party members concerned about maintaining sex-based rights and single-sex spaces ‘dinosaurs’ and accused women of ‘hoarding’ their rights? To the extent that he, an elected representative, talked over a woman, justifying it by asserting that he’s a feminist himself and berating her for not asking him about the issues that he deems more important? Is it surprising that a man who thinks a man can become a woman also thinks he can be a better feminist than a woman?
Is this a situation in which it benefits women to be nice?
Is this a situation in which women should try to be nice? I think not.
Make More Noise & Standing for Women arrange a protest
 The first I heard of it was from a message that appeared in a few of those elitist and powerful WhatsApp groups, the ones often controlled by internationally famous and wealthy lesbians, which women use to hatch our plans to overthrow the patriarchy and rule the universe. The protest was a secret, the message read, giving details and a contact…
The first I heard of it was from a message that appeared in a few of those elitist and powerful WhatsApp groups, the ones often controlled by internationally famous and wealthy lesbians, which women use to hatch our plans to overthrow the patriarchy and rule the universe. The protest was a secret, the message read, giving details and a contact…
Actually, there was also a poster advertising the event.
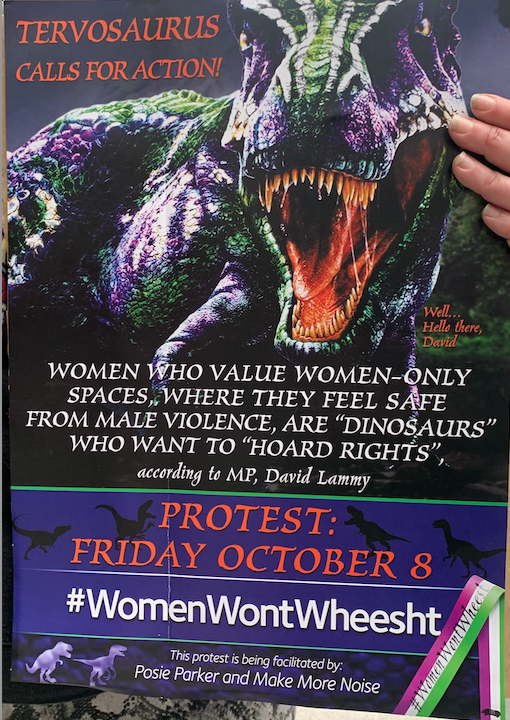
“Tervosaurus calls for action!” read the poster.
“Women who value women-only spaces, where they feel safe from male violence, are ‘dinosaurs’ who want to ‘hoard rights’ according to MP David Lammy. Protest, Friday October 8th. #WomenWontWheesht. This protest is being facilitated by Posie Parker and Make More Noise.”
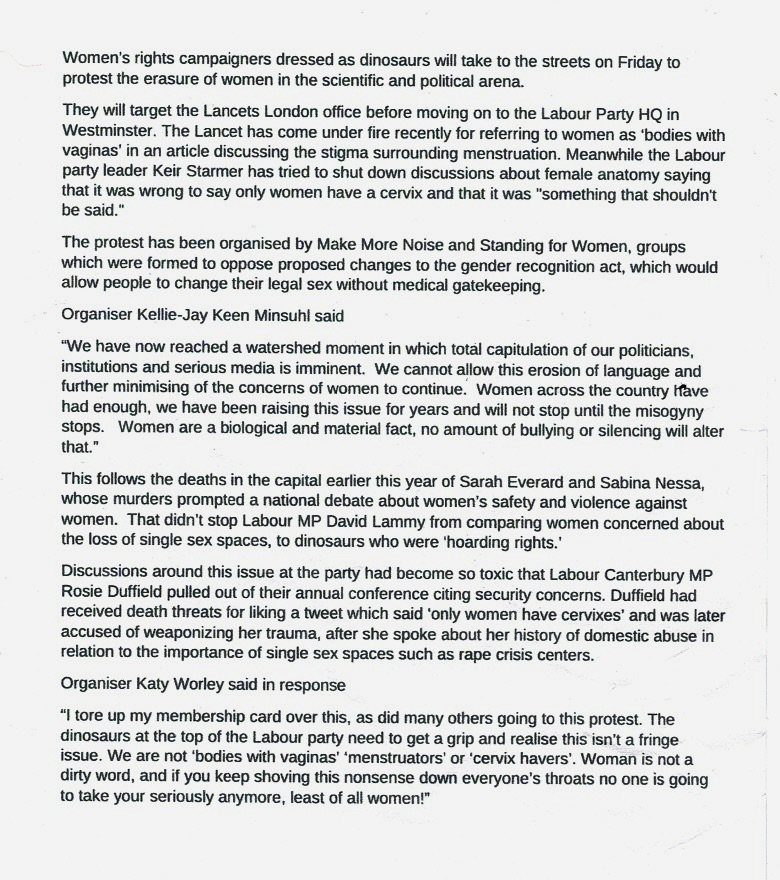
There was also a press release:
Friday dawned, a little overcast but warm. I dug out my vulva banner from behind my desk- “I thought my clitoris might have fallen off,” I confided to a friend, “but luckily it was fine”- popped it in a bin liner and headed for the station.
A group of us met outside a coffee shop in the city. The barrista was friendly and made a great cup of coffee. We tried to keep the entrance and a path along the pavement clear: now I was holding my coffee it made it difficult to juggle my bag and my placard. At one point I leaned my vulva up against the window of the fancy tailor’s shop next door. The owner was out in a flash.
“Get that sign away from my window right now, please,” he barked, brusquely.
I could see his point entirely. A posh bloke is quite likely to be daunted from entering a tailor’s for a fitting if he spies a large silk vulva propped up outside the front window.
“I’m doing that, right now,” I obliged, spilling half my coffee on the pavement.
Once it seemed like most people had arrived, we walked up and met another group who had gathered in the small square outside a nearby pub.
And it was there that I first saw the glorious dinosaurs!
Women’s rights are dino-mite

Dinosaurs sporting the colours of the suffragette flag pose for a photo in the square with Posie
There was something about the way the dinosaurs moved, the way their little arms flapped and their little butts wiggled inches from the ground. Their mouths were angled up towards the sky as if they were about to roar. They were absolutely brilliant. You can see one cross the road (safely chaperoned, of course) here.
 Our gathering had not gone unnoticed. A police officer from the City came and had a word. Some of the dinosaurs stood behind him as he chatted good-naturedly with Posie and a few others about where we were going and how long we planned to be here. Posie made it clear that she knew the law concerning the gathering and he had no problem with that.
Our gathering had not gone unnoticed. A police officer from the City came and had a word. Some of the dinosaurs stood behind him as he chatted good-naturedly with Posie and a few others about where we were going and how long we planned to be here. Posie made it clear that she knew the law concerning the gathering and he had no problem with that.
“We’re women’s right campaigners and we’re just going to give a couple of speeches and then we’ll move on.”
We saw him again a few hours later. “Who put me on Twitter?” he laughed. Pretty good sleuthing skills there from somebody in their IT department.
wait.. what… who has a cervix?

Once everyone had arrived; grabbed a coffee, gone to the loo, clambered into or out of a dinosaur suit, we walked from the square to the headquarters of The Lancet.
The Lancet was founded nearly 200 years ago and is widely considered to be one of the most respected medical journals in the world. For those of us that grew up in medical households, The Lancet commands an almost biblical reverence. Weekly, it features a selection of peer reviewed articles for the medical establishment and the layperson.
 On September 24th The Lancet tweeted “Our new issue is here! On the cover—’Periods on display’ and the cultural movement against menstrual shame and #PeriodPoverty. Plus, @WHOair quality guidelines, low #BackPain management, community-acquired bacterial #meningitis, and more”.
On September 24th The Lancet tweeted “Our new issue is here! On the cover—’Periods on display’ and the cultural movement against menstrual shame and #PeriodPoverty. Plus, @WHOair quality guidelines, low #BackPain management, community-acquired bacterial #meningitis, and more”.
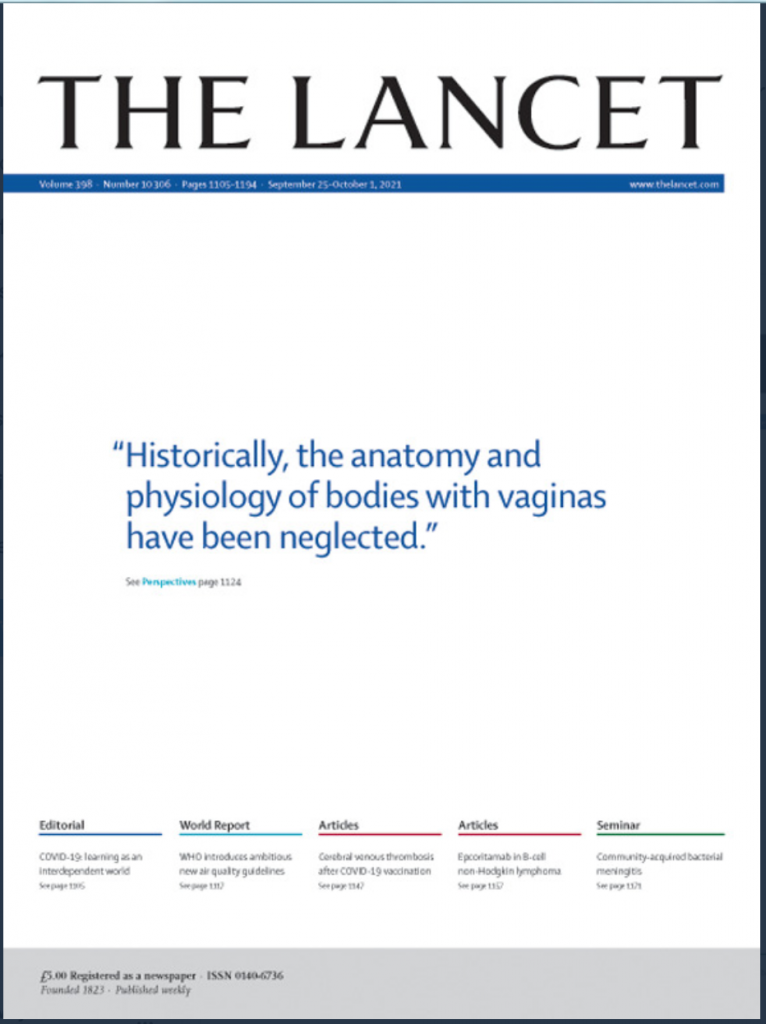
And more. Those two little words there at the end became most significant- because what everybody ended up talking about was the headline on the cover of the magazine rather than the content of the articles inside. The headline read:
“Historically, the anatomy and physiology of bodies with vaginas have been neglected.”
 Yet just a week beforehand the Lancet had advertised a seminar where they had no issue with naming the sex of the owner of a different organ. ‘About 10 million men are currently living with a diagnosis of prostate cancer—making it a major health issue’ the blue tick account tweeted.
Yet just a week beforehand the Lancet had advertised a seminar where they had no issue with naming the sex of the owner of a different organ. ‘About 10 million men are currently living with a diagnosis of prostate cancer—making it a major health issue’ the blue tick account tweeted.
It appears that the woowoo is only to be indulged when women’s bodies are under scrutiny.
The Lancet HQ is on the corner of a busy junction in the city. Most of us stood outside the main building, with others scattered on the corners of the junction and on the other side of the crossing you see here. You can see some of the livestream here on Posie’s YouTube Channel.
“Only women have a cervix! Only men have a penis!”

 How many of us were there ? Well, the cop who spoke to us in the square estimated our numbers at about forty. More people joined us after that point: there are 58 protestors in this picture (I zoomed in on ‘photos’ to headcount) and about a dozen more on the other side of the road and at the junctions.
How many of us were there ? Well, the cop who spoke to us in the square estimated our numbers at about forty. More people joined us after that point: there are 58 protestors in this picture (I zoomed in on ‘photos’ to headcount) and about a dozen more on the other side of the road and at the junctions.
People came and went but I’d guess there were 70+ of us at this point, which when you consider the fact that it was short notice & a weekday, leaving many women with work and childcare obligations- not to mention the potential implication of publicly standing up for sex-based rights- is a pretty damn good turn out IMO.
Here are some of the banners.



The road facing us was busy and numerous cars, buses and lorries honked their support – although many of them probably didn’t have the foggiest idea what they were honking at. Dinosaurs, though! What’s not to like?
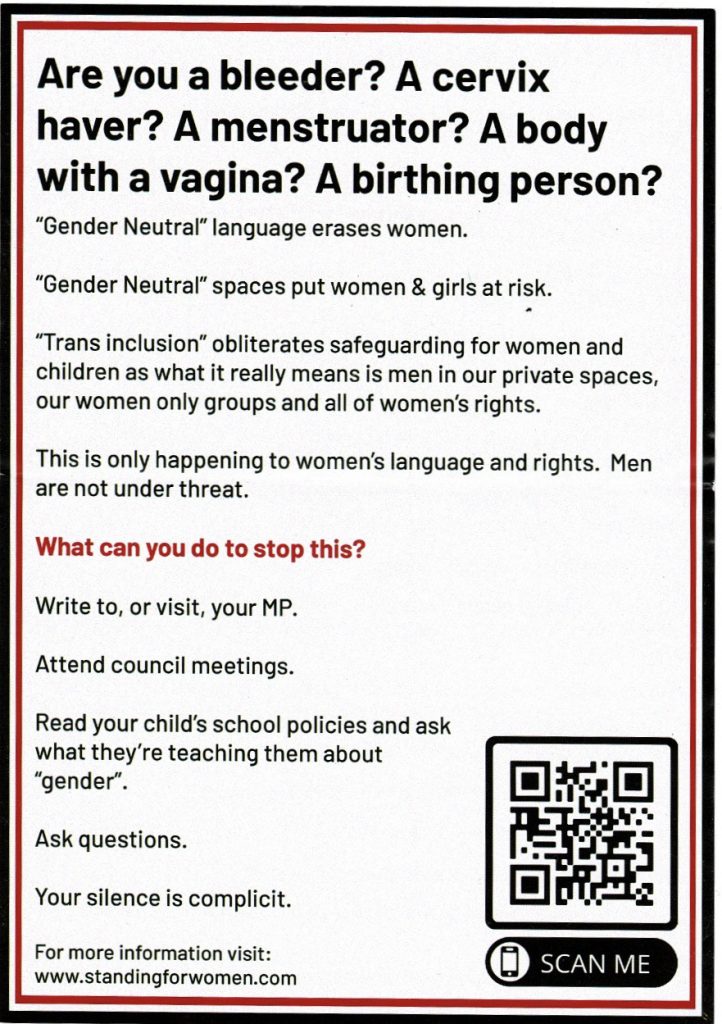
The protestors handed out two types of leaflet. The larger of the two was from Standing for Women, a double-sided A5 sheet like this:
![]()
The second leaflet was half the size. It had been produced by Essex Resisters and featured a picture by The Famous Artist Birdy Rose. It looked like this:
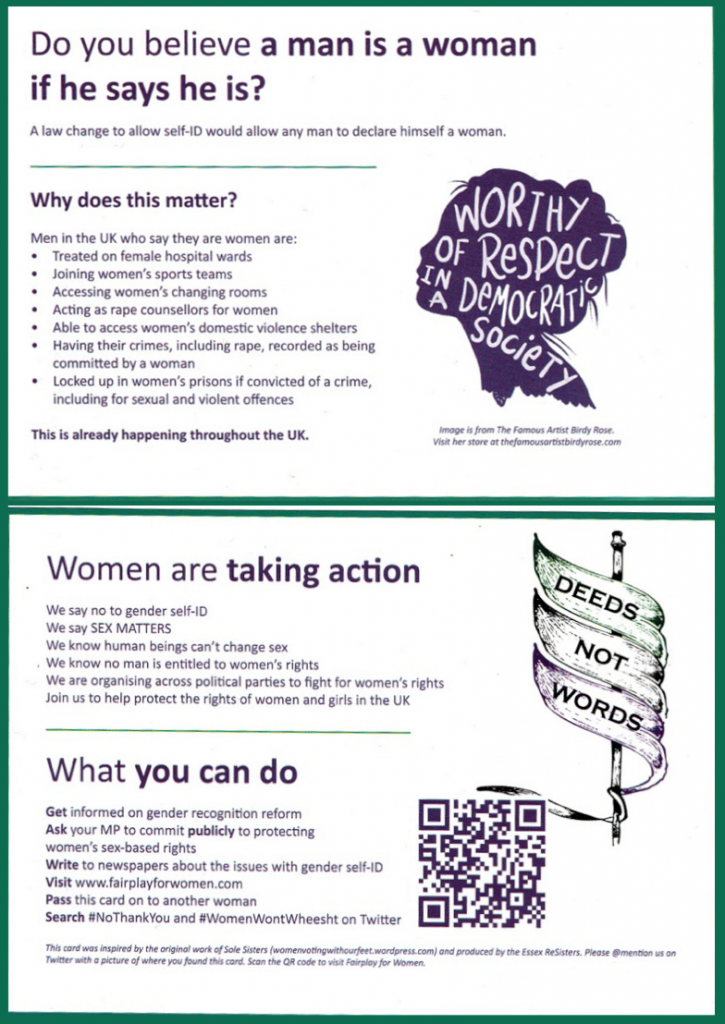
Most people who were offered a leaflet took one; some passers by stopping to chat and ask questions: sometimes about the leaflets – and sometimes about the dinosaurs.
I t was outside The Lancet that one dinosaur & Mr Memo performed the impromptu song and dance routine that has triggered transactivists everywhere.
t was outside The Lancet that one dinosaur & Mr Memo performed the impromptu song and dance routine that has triggered transactivists everywhere.
I had been taking a series of photos and short videos and said to them, ‘Oh go on, give us a song and a dance!’
So they obliged and performed a brief rendition of ‘if a person has a penis he’s a man’. The result is, in my humble opinion, hilarious and you can see it here.
One thing that struck me about the responses of TRAs is how horrified they seemed to be on our behalf: a bit like an adolescent child who has caught their drunk dad dancing at a party. Over & again they recoiled from the “embarrassing, depressing, awful dancing” talking about it as if it had been produced for an X Factor audition. They just didn’t get that it wasn’t meant to be impressive. It was as if they somehow thought Dino & Memo were trying to be cool. “It’s so embarrassing,” they kept commenting. Perhaps when you spend your entire life taking yourself very, very seriously, you lose the ability to appreciate that others don’t do the same?
“GC people having a blast making David’s lemons into lemonade… TRAs are total killjoys but they can’t stop the dinos making us happy. It’s just not possible!“ tweeted one Twitter user happily.
We stayed outside The Lancet offices for about an hour before walking up to Mansion House and taking the tube up to Westminster, where we regrouped by the Millicent Fawcett statue. Some people had to leave and others joined us. Those who didn’t mind appearing in a photo posed in front of the statue for this picture.

In front of the Fawcett statue – photo by Mr Memo
At the statue there were chants and speeches, and some general milling around. You can see some footage from Parliament square here.
 “Over there in those lovely Victorian buildings,” Posie gestured towards the Houses of Parliament, “Parliamentarians refuse to say a woman is an adult human female.”
“Over there in those lovely Victorian buildings,” Posie gestured towards the Houses of Parliament, “Parliamentarians refuse to say a woman is an adult human female.”
The crowd booed.
I took the opportunity to chat with some other protestors and get their thoughts on the day. These are some of the reasons they gave for attending.
Giving & getting support
“I’m really happy to unite and hang out with like-minded women. I feel like being gender critical is sometimes frowned upon, so I feel supported and loved here and I’d encourage any woman with any ounce of critical thinking or compassion for other women, to come and support ‘Standing for Women’.”
Don’t conflate sex with gender
“Stop using female words for men you like, please people, because that conflates sex with gender and when you conflate sex with gender that’s when women lose their single-sex spaces. So please don’t do it. Thank you!”
Right side of history
“We just met some girls from a very privileged school: we think they were <name of school redatcted> girls, and they were telling us that we were hateful and transphobic for not accepting people’s gender identity. And I told them in ten or even five years’ time they’ll look back on today and they’ll realise how wrong they were. They’re being gaslit. Whoever told him that transwomen were actually women was lying to them- and in whose interest is that?”
Boosting morale
“I don’t know, I guess I just like helping with morale. It shows that at least someone who’s kind of a semi fake celeb sees that this is all nonsense, and insanity, homophobia and misogyny all wrapped up in one big bundle.”
We need to be able to tell what a woman is
“The classification of women as a sex-based protected class is important. It’s important medically, it’s important biologically, it’s important legally, it’s important historically; archaeologically- in every way it’s important to be able to tell what a woman is! To be able to classify what a woman is, and if we can’t do that we lose so much- and that’s why we’re here today.”
Autistic kids
“I’m here today because I’m an autistic man and autistic children are often the most captured by the trans cult, especially autistic girls because sometimes they are naturally a bit more gender nonconforming than everyone else, or they feel different from others. They may have problems like anorexia or bulimia, and transgenderism is like the new thing for these people.”
“I’m a woman from Bristol, I’m a bisexual woman I’ve been told many times that my sexuality is now ‘invalid’. I have a young girl who is an autistic gender non-conforming child and I fear for the world she is growing up in now. Women are losing their rights every day and it’s very difficult to bring your child up in this world.”
The Sikh influence
“When Maharaja Ranjit Singh, who was deposed in Punjab lost his Kingdom, his 10 year old son was brought here to be bought up by Queen Victoria. That son’s daughter was the suffragette Sophia Duleep Singh, so there have been Sikhs involved in the suffragette movement since the inception of the suffragettes,” I was told by a woman who had been raised in the Sikh faith. “So I feel like it’s my duty to be here representing that aspect of the suffragettes.”
Standing up for lesbians & same-sex attraction
“I’m here because I’m a lesbian- a lesbian not LGBTQXXXX+++! They’ve got no right to say that I’m part of their group, I’m not. A woman is an adult human female and I am single-sex attracted to other adult human females. Men are not women. That is it.”
a privileged belief system
I’d like some people to know that they’ll never be forgiven. People like Owen Jones- anybody who’s been on board with this. Anybody who’s got a brain and has cheerled for this; anybody who has cancelled women; who’s made my life difficult. I’m nobody. I’m just a cleaner from Sheffield, I’m an absolute nobody and my life is more difficult because of rich wankers who’ve got a privileged belief system: a privileged belief system that has no reality to it at all.”
Men can fuck off
“I’ve got something to say,” said one woman, popping up beside me. “Men can fuck off.” And then she was gone.
After some time milling around and making speeches at Parliament Square, it was time to head to Labour Party Headquarters. So off we went.
The Cervix Wars
 In August, Labour MP Rosie Duffield became embroiled in the cervix wars after ‘liking’ a tweet. Yes, there really are people who trawl Twitter, checking which Tweets certain people have ‘liked’- behaviour which TBH makes walking round London in an inflatable dinosaur suit chanting “only women have cervixes” look like positively pedestrian behaviour.
In August, Labour MP Rosie Duffield became embroiled in the cervix wars after ‘liking’ a tweet. Yes, there really are people who trawl Twitter, checking which Tweets certain people have ‘liked’- behaviour which TBH makes walking round London in an inflatable dinosaur suit chanting “only women have cervixes” look like positively pedestrian behaviour.
To cut a long story short, CNN tweeted that ‘individuals with a cervix’ should get screened once they reached the age of 25, Piers Morgan commented ‘Do you mean women?’, Rosie Duffield ‘liked’ the tweet and as the floodgates of righteous indignation opened the accusations of transphobia flowed thick and fast.

The Labour Campaign for Trans Rights announced that it was ‘shocked and saddened’ and called for action. Duffield initially appeared astonished.
Suddenly, everybody was talking about cervixes.
Did Kier Starmer stand by Rosie Duffield? Did he fuck.
Starmer not only ignored calls to defend Rosie but when asked on the Andrew Marr Show if it was transphobic to say ‘only women have a cervix’ he replied:
“Well, it is something that shouldn’t be said. It is not right.”
Shadow chancellor Rachel Reeves was put on the spot by Ferrari, who asked her the same question that had been asked of Starmer and Lammy: “Is it transphobic to say ‘only women have a cervix’?“
Reeves appeared flustered and uncomfortable. After calling the issue ‘devisive and toxic’ and the debate ‘unhelpful and unproductive’, a breathless and gasping Rachel managed “I just don’t even know how to start answering these questions.”
Repeating with confidence only the mantra that men or women should be able to identify however they wanted ‘whatever their body parts’, it was disconcerting to watch a flustered and uncomfortable Reeves squirm under the stern eye of Ferrari. It was as if she were genuinely terrified that he might see into her innermost soul and declare her to be Anti Trans.
Because we all know what that would mean.
“Our traditional take on gender no longer works,” coos Jane Faye in the Independent. “Many trans women continue to have a prostate, despite surgeries on other more sensitive areas. Many trans men have cervixes. Non-binary folk may have either. Or neither. Which is true of the general population, too.”
What the very fuck is this disingenuous nonsense? This is not about a ‘traditional take’ on gender. It’s not about gender at all. It is about sex. Biology. Biological sex. The gender fairy does not randomly strew cervixes throughout the general population. The cervix is not a fashion accessory. It’s an important part of a woman’s reproductive system. Your cervix doesn’t care about your gender identity and it should be of little or no relevance to your gynecologist either.
But I digress.


Labour party headquarters is a modern, glassy building not far from Victoria Station, with a spacious paved square in front.
More speeches took place, and some chanting and whistle-blowing.
The dinosaurs, who had already excelled themselves, suddenly produced a batch of eggs and began arranging a small nest at the side of the main glass windows. Each egg was fashioned from papier maché built up around a balloon, and each egg had something written on it.
I managed to catch up with DJ Lippy, who designed the eggs, and ask her about their significance.
“I made the eggs as official representation of the rights we’re going to lose,” she told me. “It’s quite difficult for people to understand, so we’ve broken them down because it does seem quite esoteric unless you’re in the know and you’ve done a bit of research. I wanted to make some eggs because we’re told we were hoarding our rights and I thought ‘what does a dinosaur  hoard?’ Well, a dinosaur hoards eggs! so I just thought I’d use it. Each egg has a different right that women are losing: there’s lesbian rights for example: lesbians are now not allowed to define themselves as same-sex attracted and neither are gay men. Then we’ve got female only changing rooms: if you’ve heard about the Wii Spa incident you can see the problems caused by current legislation. Women only prisons: men have been transferred to women’s prisons- rapists and sex offenders and dangerous sexual predators in some cases. They should not be in the female estate. Accurate crime statistics: so if you’re allowed to self-identify yourself when you commit a crime then loads of rapists are identifying as women and that’s skewing the crime statistics. I’m gonna do a little speech about it all in a minute…”
hoard?’ Well, a dinosaur hoards eggs! so I just thought I’d use it. Each egg has a different right that women are losing: there’s lesbian rights for example: lesbians are now not allowed to define themselves as same-sex attracted and neither are gay men. Then we’ve got female only changing rooms: if you’ve heard about the Wii Spa incident you can see the problems caused by current legislation. Women only prisons: men have been transferred to women’s prisons- rapists and sex offenders and dangerous sexual predators in some cases. They should not be in the female estate. Accurate crime statistics: so if you’re allowed to self-identify yourself when you commit a crime then loads of rapists are identifying as women and that’s skewing the crime statistics. I’m gonna do a little speech about it all in a minute…”
and she was gone.
Passers by stopped, some listened, several children were entranced by the dinosaurs. A delivery man passing through the crowd snorted.
“Men being women? Yeah, and gravity doesn’t exist either!” he scoffed, and looked both surprised and rather proud when he received a round of applause and a burst of whistle blasts in appreciation.
“I’ve got a message for Keir Starmer,” announced Posie through the megaphone. “Dear Mr Starmer. Labour is losing women. We stand with Rosie Duffield. The absolute disgrace of the Labour Party is that female MPs don’t even feel safe enough to go to the party conference.”
“Labour,” she added, sternly, “is losing so many women that you think they’d know what one is by now.’
Around four o’clock we decided to wind things up. People were getting hungry and we had our eyes on a nearby pub for drinks and snacks. I detached the bamboo support pole from my banner and popped my vulva back into its bin liner. It’s now safely back behind the desk in my workshop, waiting for its next adventure.
So that’s the tale of Friday’s protest, really. Megaphone & whistles, banners and masks, vulvas and dinosaurs, ribbons and placards.
Camaraderie and a sense of hopeful determination.
As for the idea that ‘dinosaurs were stupid and they became extinct’ I’d like to point out that current thinking holds that the dinosaurs were evidently doing very well, thank you, until a bloody great asteroid smashed into the planet.
If only they could have identified as tardigrades.

 Of course you’re not ‘assigned a gender’ at birth- but you will be subject to stereotyping from the moment you’re born.
Of course you’re not ‘assigned a gender’ at birth- but you will be subject to stereotyping from the moment you’re born. The problem, of course, is not with the child who doesn’t play the gender game easily but with the fact that adhering to these gendered stereotypes is one of the things that helps kids- that helps all of us- ‘fit in’. And therein lies the problem. ‘Being trans’ offers the child who is having trouble negotiating gender a way of being special and fitting in at the same time. ‘Being trans’ also tells the kid that there’s something wrong with them that needs fixing.
The problem, of course, is not with the child who doesn’t play the gender game easily but with the fact that adhering to these gendered stereotypes is one of the things that helps kids- that helps all of us- ‘fit in’. And therein lies the problem. ‘Being trans’ offers the child who is having trouble negotiating gender a way of being special and fitting in at the same time. ‘Being trans’ also tells the kid that there’s something wrong with them that needs fixing. 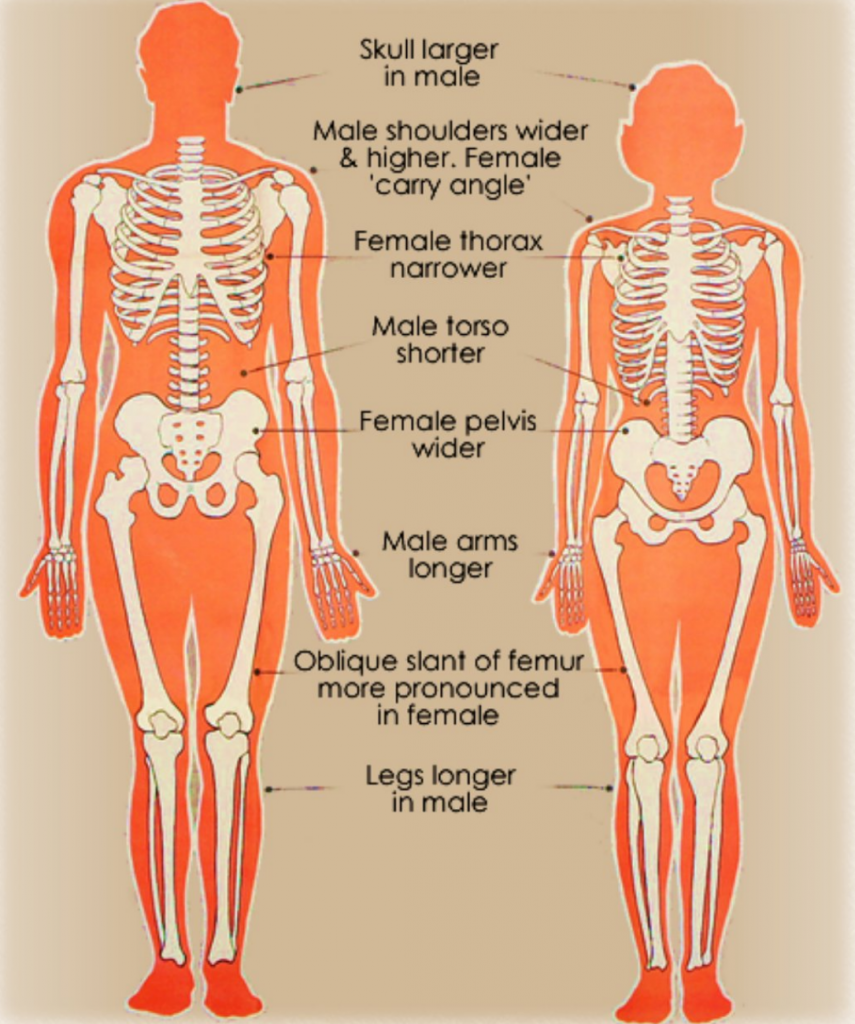 We could start by celebrating female athletes and their achievements. Teach kids about the differences between male and female bodies, and why women and girls need single sex sports because of those differences. Teach them to celebrate and respect those differences.
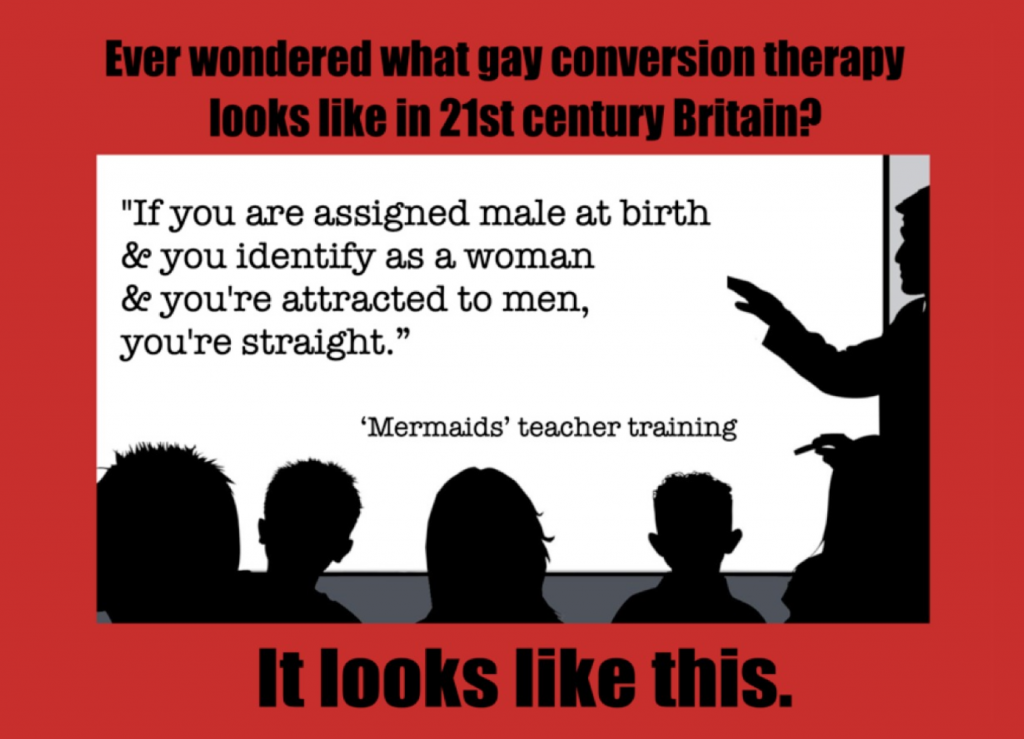
We could start by celebrating female athletes and their achievements. Teach kids about the differences between male and female bodies, and why women and girls need single sex sports because of those differences. Teach them to celebrate and respect those differences.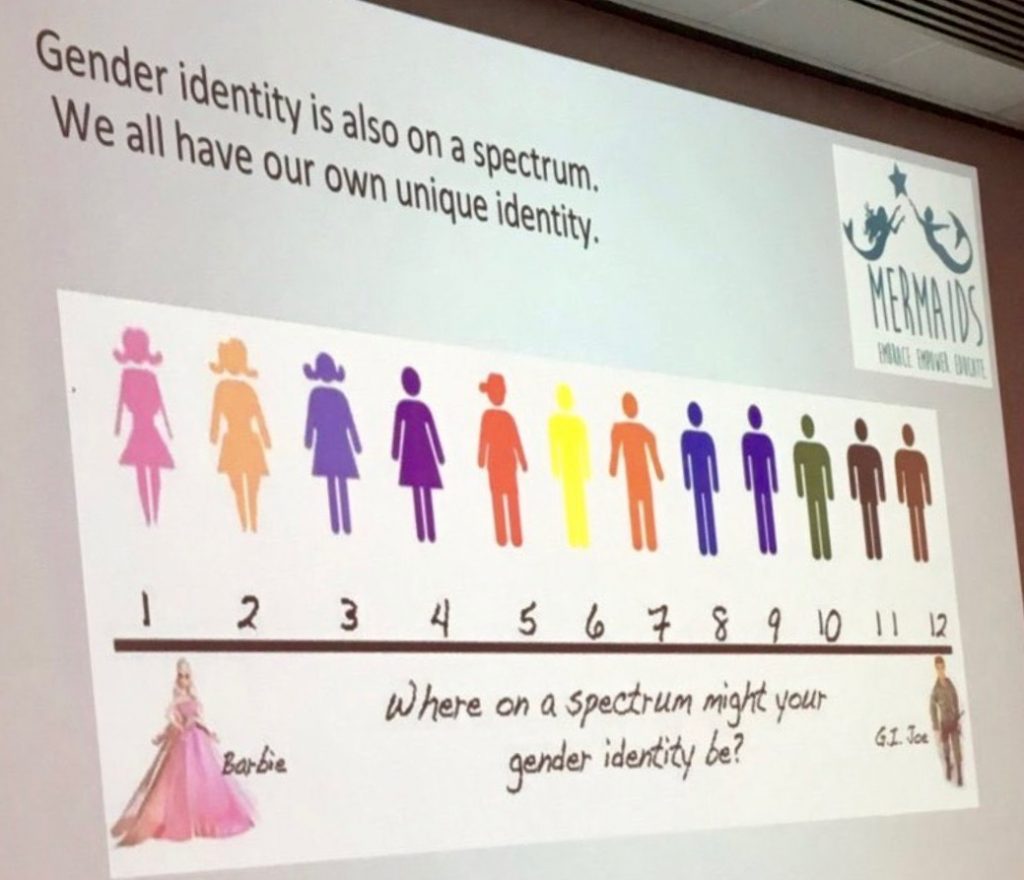 The famous ‘are you Barbie or GI Joe’ Mermaids training slide is not just a little slither of harmless madness. It teaches that a real 100% girl identity is Barbie. A real 100% boy identity is GI Joe.
The famous ‘are you Barbie or GI Joe’ Mermaids training slide is not just a little slither of harmless madness. It teaches that a real 100% girl identity is Barbie. A real 100% boy identity is GI Joe.